20 LEI
MEDICAL CONNECTIONS
CONEXIUNI MEDICALE
THE JOURNAL
OF PHYSICIANS from Satu Mare County
REVISTA CORPULUI MEDICAL SĂTMĂREAN publicată de Colegiul Medicilor Satu-Mare
PARTNERS / PARTENERI:
Titu Maiorescu University Bucharest
Faculty of Medicine and Dental Medicine,
Hasharon Hospital, Rabin Medical Center,
affiliated with Sackler School of Medicine,
Tel Aviv University
Vasile Goldiş Western University of Arad
Included in The Schedule of Medical Publications of CMR
Indexed in Journals Master List of Index Copernicus®
CNCSIS B+ Category, Code 944
ISSN 1843 - 9306
Volume 9 Nr. 1 (33)
MARCH 2014
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
ASSISTANT EDITORS
EDITOR IN CHIEF
Blaga Vasile (electronic version)
Koren Rumelia
Andó Ottó (print version)
ASSISTANT EDITOR IN CHIEF
Oană Cristian Sever (editorialist)
Bumbulu Călin
Stăncioiu Tudor (Dental Medicine)
EDITORIAL BOARD
Bauer Adalbert (SCM Satu Mare, România)
Lup Liliana (Synevo Satu Mare, România)
Bidilean Nicolae (Emergency County Hospital,
Kesler Gavriel (Israel)
Satu Mare, România)
Kiss Ladislau (Emergency County Hospital,
Boros Melinda (Bucureşti, România)
Satu Mare, România)
Borcean Gheorghe (Caransebeş Hospital, România)
Mihalca Man Sorina (Emergency County Hospital,
Brândeu Ioan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Neumann Gad (Hasharon Hospital, Tel Aviv, Israel)
Cârstea Constantin (CMI Braşov, România)
Negru Alina (SCM Satu Mare, România)
Cojocaru Manole (Titu Maiorescu University,
Rath-Wolfson Lea (Hasharon Hospital, Tel Aviv, Israel)
Bucureşti, România)
Rădulescu Viorel (CMI Olt, România)
Comăneanu Raluca Monica (Titu Maiorescu University,
Roatiş Marius Dinu (Emergency County Hospital,
Bucureşti, România)
Satu Mare, România)
Cornean-Santa Corina (Emergency County Hospital,
Rusu Cristian Bogdan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Feciche Bogdan (Emergency County Hospital,
Shvero Kesler Dana (Hadassa University, Jerusalem, Israel)
Satu Mare, România)
Trip Gheorghe (Emergency County Hospital,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Hasharon Hospital,
Zilahi Karoly (SCM Praxis, Bixad, România)
Tel Aviv, Israel)
Zeidman Aliza (Hasharon Hospital, Tel Aviv, Israel)
Horber Orsolya (SCM Praxis Bixad, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
ASSOCIATED EDITOR
College of Physicians Satu Mare
Satu Mare Association of Family Physicians
Satu Mare, 23 Eroilor Revolu iei Pl.
A liated with National Society of Family Medicine/
General Medicine
email: colmedsm@gmail.com
Satu Mare, UK 30 Bobocului St.
PARTNERSHIP
EXTERNAL PARTNERSHIP
Titu Maiorescu University, Bucharest
Vasile Goldiş
Hasharon Hospital,
Faculty of Medicine and Dental Medicine
Western University of Arad
Rabin Medical Center
67A Gheorghe Petraşcu St.
94 Revolutiei Blvd., Arad, Romania
A liated with Sackler School of Medicine,
Petah Tikva 49372, Israel
EDITORIAL OFFICE
23 Eroilor Revolu iei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Journal included in e Schedule of Medical Publications of CMR, 5 credits CMR for subscribers
Indexed in Index Copernicus®, CNCS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family Physicians
Printed at TIPOOFFSET, Fabricii st, No. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIIN IFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu
Prof. Univ. Dr. Tuvia Hadar
(Emergency County Hospital, Satu Mare,
(Beilinson Hospital, Rabin Medical Center, Sackler
Romania)
Faculty of Medicine, Tel Aviv University, Israel)
Acad. Prof. Univ. Dr. Doina Onicescu
Prof. Univ. Dr. Gheorghe Manole
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Sorin Riga
Prof. Univ. Dr. Dorel Augustin Manu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Dan Riga
Prof. Univ. Dr. Dan Mănăstireanu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Vasile Astărăstoae
Prof. Univ. Dr. Elena Moldoveanu
(Gr. T. Popa University of Medicine and Pharmacy,
(Titu Maiorescu University, Faculty of Medicine
Iaşi, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rumelia Koren
Prof. Univ. Dr. Adriana Stănilă
(Hasharon Hospital, Rabin Medical Center, Sackler
(Victor Papilian Faculty of Medicine, Sibiu,
School of Medicine, Tel Aviv University, Israel)
Romania)
Prof. Univ. Dr. Petru Armeanu
Prof. Univ. Dr. Maria Lidia Nica Udangiu
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin
Prof. Univ. Dr. Dan Florin Ungureanu
(Victor Babeş University, Faculty of Medicine,
(Titu Maiorescu University, Faculty of Medicine
Timişoara, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa
Conf. Univ. Dr. Ghinescu Minerva
(Ovidius University, Constan a, Romania)
(Titu Maiorescu University, Bucureşti, România)
Prof. Univ. Dr. Constantin Dumitru
Conf. Univ. Dr. Mircea Sorin Sabău
(Titu Maiorescu University, Faculty of Medicine
(University of Medicine and Pharmacy Târgu
and Dental Medicine, Bucharest, Romania)
Mureş, Romania)
Prof. Univ. Dr. Rivka Gal
Ş. L. Dr. Anca Ciurea
(Hasharon Hospital, Rabin Medical Center, Sackler
(Iuliu Ha ieganu University, Faculty of Medicine,
School of Medicine, Tel Aviv University, Israel)
Cluj Napoca, Romania)
Prof. Univ. Dr. Doina Lucia Ghergic
Ş. L. Dr. Virgil Radu Enătescu
(Titu Maiorescu University, Faculty of Medicine
(Eduard Pam l Universitary Clinic of Psychiatry,
and Dental Medicine, Bucharest, Romania)
Timişoara, Romania)
e Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
CNCS B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2014
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any
means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is
shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: colmedsm@gmail.com
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
EDITORI ADJUNC I
EDITOR ŞEF
Blaga Vasile (versiunea electronică)
Koren Rumelia
Andó Ottó (versiunea tipărită)
EDITOR ŞEF ADJUNCT
Oană Cristian Sever (editorialist)
Bumbulu Călin
Stăncioiu Tudor (Medicina Dentară)
COMITET EDITORIAL
Bauer Adalbert (SCM West Satu Mare, România)
Kesler Gavriel (Israel)
Bidilean Nicolae (Spital Jude ean de Urgen ă,
Kiss Ladislau (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Boros Melinda (Bucureşti, România)
Mihalca Man Sorina (Spital Jude ean de Urgen ă,
Borcean Gheorghe (Spital Municipal Caransebeş, România)
Satu Mare, România)
Brândeu Ioan (Spital Jude ean de Urgen ă,
Neumann Gad (Spital Hasharon, Tel Aviv, Israel)
Satu Mare, România)
Negru Alina (SCM Satu Mare, România)
Cârstea Constantin (CMI Braşov, România)
Rath-Wolfson Lea (Spital Hasharon, Tel Aviv, Israel)
Cojocaru Manole (Universitatea Titu Maiorescu,
Rădulescu Viorel (CMI Olt, România)
Bucureşti, România)
Roatiş Marius Dinu (Spital Jude ean de Urgen ă,
Comăneanu Raluca Monica (Universitatea Titu Maiorescu,
Satu Mare, România)
Bucureşti, România)
Rusu Cristian Bogdan (Spital Jude ean de Urgen ă,
Cornean-Santa Corina (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Shvero Kesler Dana (Universitatea Hadassa,
Feciche Bogdan (Spital Jude ean de Urgen ă,
Ierusalim, Israel)
Satu Mare, România)
Trip Gheorghe (Spital Jude ean de Urgen ă,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Spital Hasharon, Tel Aviv, Israel)
Zilahi Karoly (SCM Praxis, Bixad, România)
Horber Orsolya (SCM Praxis Bixad, România)
Zeidman Aliza (Spital Hasharon, Tel Aviv, Israel)
Lup Liliana (Synevo Satu Mare, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
EDITOR ASOCIAT
Colegiul Medicilor Satu Mare
Asocia ia Medicilor de Familie Satu Mare
Satu Mare, P- a Eroilor Revolu iei nr.23
A liată la Societatea Na ională de Medicina Familiei/
Medicină Generală
email: colmedsm@gmail.com
Satu Mare, str. Bobocului UK 30
PARTENER
PARTENER EXTERN
Universitatea Titu Maiorescu Bucureşti
Universitatea de Vest Vasile Goldiş
Hasharon Hospital, Rabin Medical Center
Facultatea de Medicină şi Medicină Dentară
din Arad
A liat la Sackler School of Medicine,
str. Gheorghe Petraşcu 67A
94 Revolu iei Blvd., Arad, România
Universitatea Tel Aviv
7 Keren Kayemet St.,
Petah Tikva 49372, Israel
REDAC IA
P- a Eroilor Revolu iei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Revistă inclusă în Nomenclatorul Publica iilor Medicale ale CMR, 5 credite CMR pentru abona i
Indexare în Index Copernicus®, CNCS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asocia iei Medicilor de Familie Satu Mare
Tipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
Contents
EDITORIAL
7
ORIGINAL ARTICLES
Detection of IgG Anti-Laminin-1 Antibodies in Patients with Acute Ischemic Stroke
Manole Cojocaru, Elena Rusu, Inimioara Mihaela Cojocaru, Isabela Siloși
9
e Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
Carmen Gheorghe, Lelia Mihai, Ioanina Parlatescu, Șerban ovaru, Elena Coculescu
13
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
Gheorghe Nicolae Sârbu, Lorant Kiss, Alina Bereanu, Roland Kiss, Dan Maniu
19
Treatment of Nocturia in a Male Group of Patients with Lower Urinary Tract Symptoms (LUTS).
Short-term Results
Vasile Dan Stanca, Andrei Boc, Radu Aurel Maxim, Vitalie Gherman, Sergiu Nicolescu, Ioan Coman
27
Finite Element Analysis of a New Expandable Interbody Fusion Cage
Mihai Magureanu, Dinu Vermesan, Juganaru Iulius, Horia Haragus, Roberta Cecilia Avram, Dan Ioan Stoia,
Gigi Adrian Aiordachioaie
31
Appendectomy in Obese People. Classic or Laparoscopic Approach?
Marius Sfîrlea, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Codru a Macovei, George Dejeu,
Ciprian Borza, Daniela Berdea, Daniela Rahotă
37
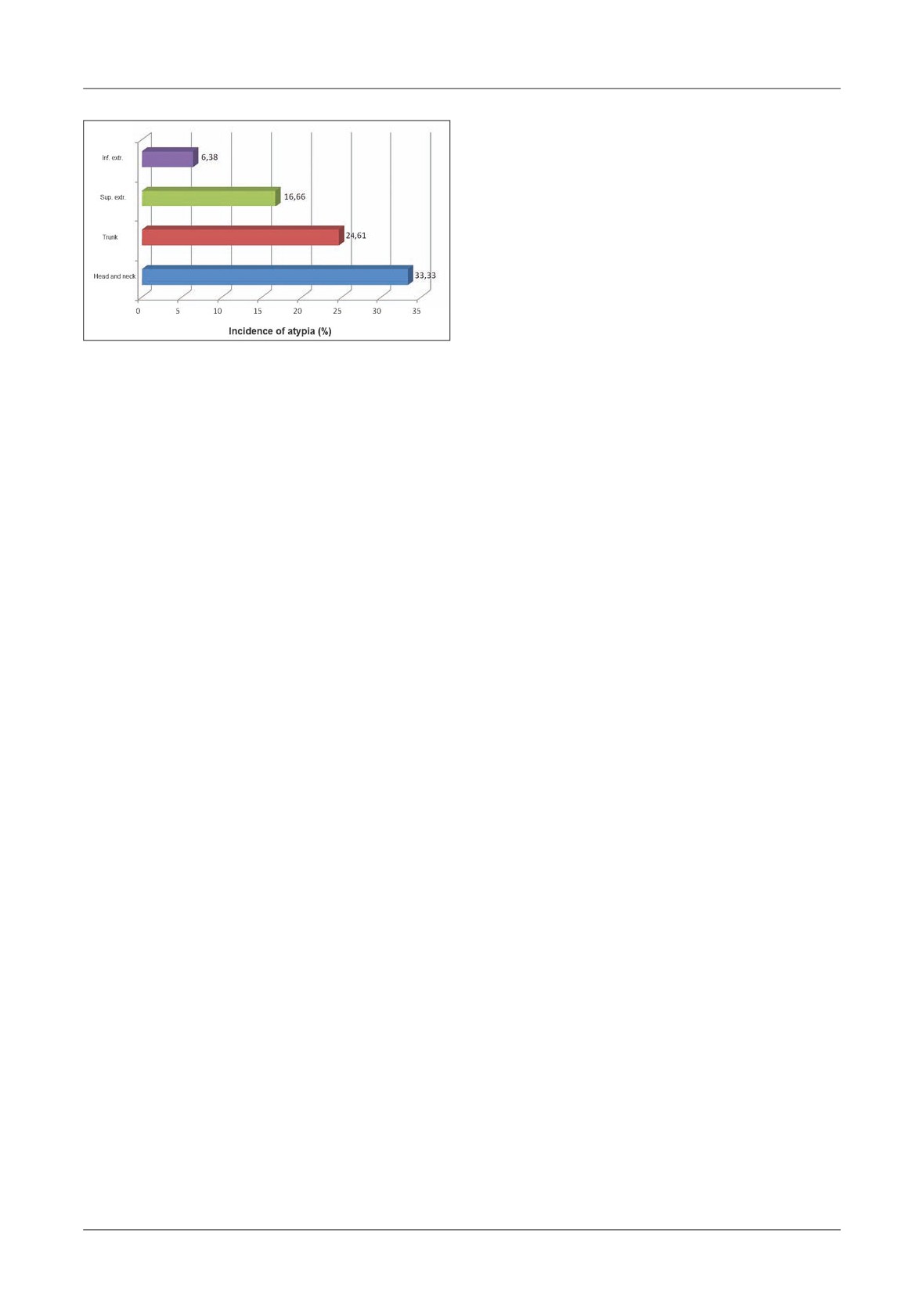
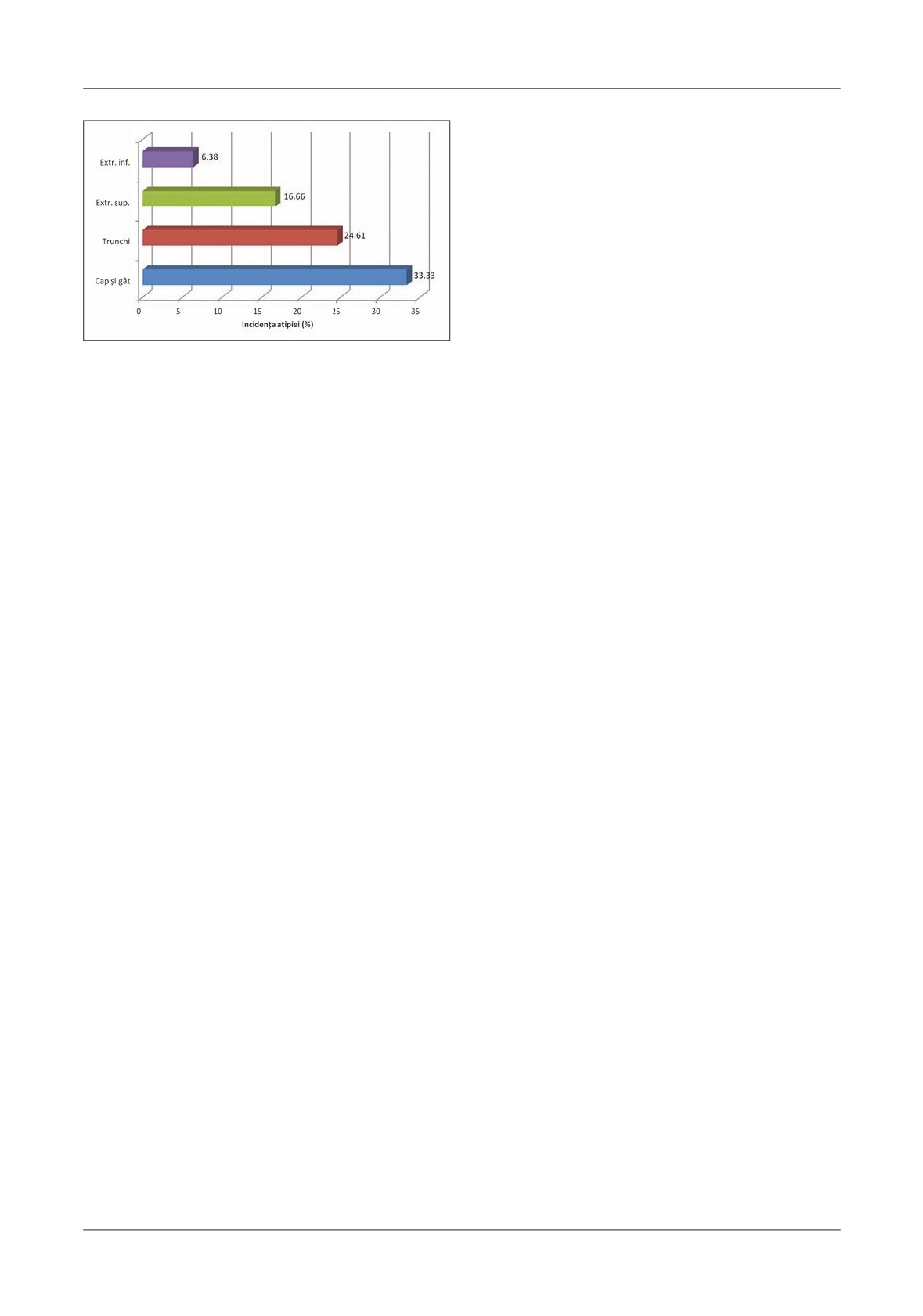
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
Florin Suru, Adrian Maghiar
43
CASE PRESENTATION
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Leukemia. Case Report
and Review of the Literature
Boris Solun, Dana Marcoviciu, Yulia Belnik, Avraham Sendovski, Dror Dicker, Ana Tovar
49
Bladder Lithiasis Secondary to a Migrated Intrauterine Device. Case Report
Victor Ona, Bogdan Feciche, Andrei Boc, Dan Ona, Ioan Coman
55
MEDICINE AND ART
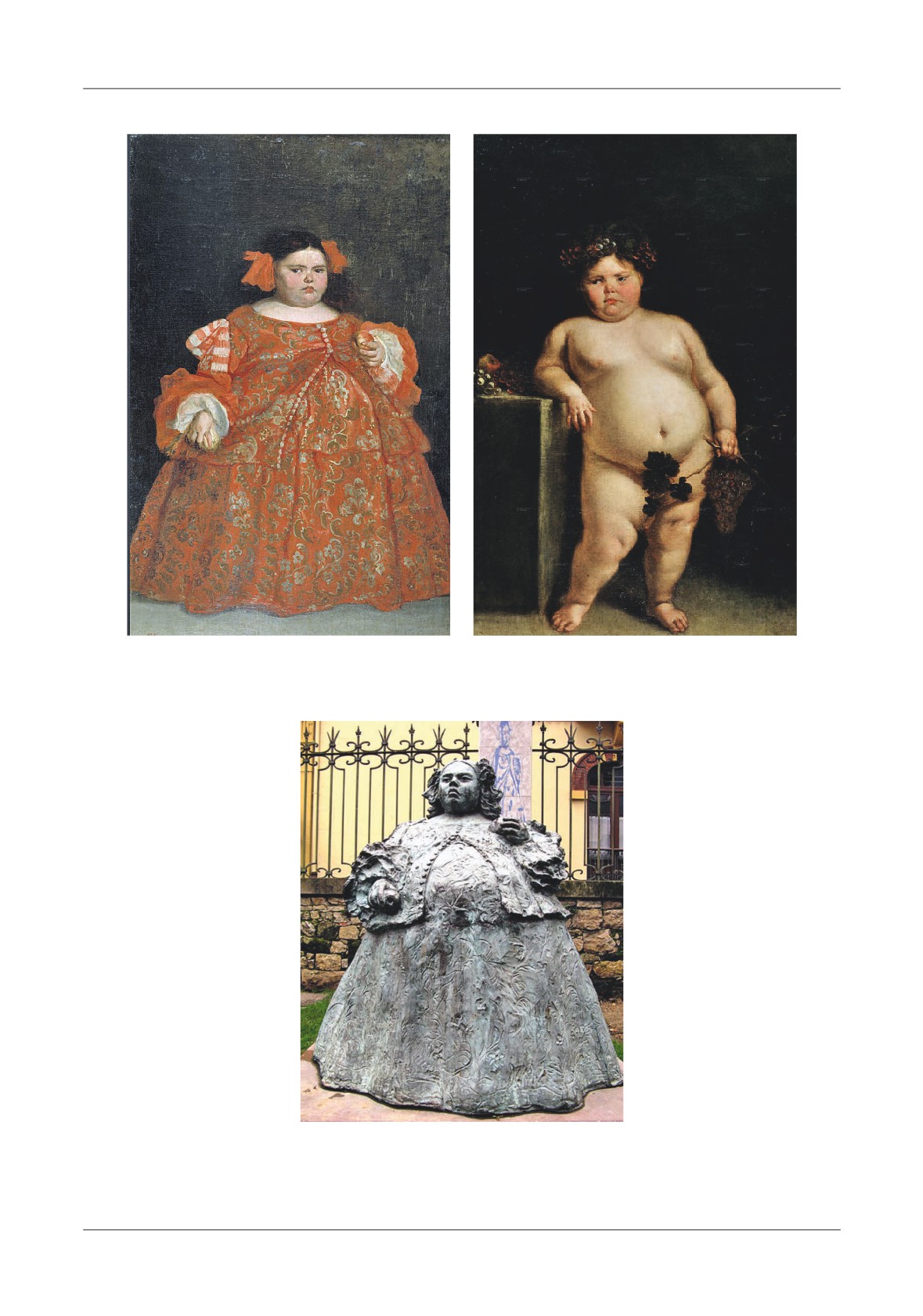
Paintings of a Case of Obesity in the 17th Century, Probably Due to Prader-Willi Syndrome
Călin Bumbulu , Andrei Bumbulu , Alina Daniela Negru, Rumelia Koren
59
GUIDANCE FOR AUTHORS
63
Cuprins
EDITORIAL
67
ARTICOLE ORIGINALE
Detectarea anticorpilor anti-laminin-1 din clasa IgG la pacien i cu stroke ischemic acut
Manole Cojocaru, Elena Rusu, Inimioara Mihaela Cojocaru, Isabela Siloși
69
Asocierea lichenului plan bucal cu hepatita cronică cu virus C. Studiu retrospectiv
Carmen Gheorghe, Lelia Mihai, Ioanina Parlatescu, Șerban ovaru, Elena Coculescu
73
Aspecte clinice și tomogra ce (CT) ale complica iilor pancreatitei acute
Gheorghe Nicolae Sârbu, Lorant Kiss, Alina Bereanu, Roland Kiss, Dan Maniu
79
Tratamentul nocturiei la un grup de pacien i de sex masculin având simptomatologie de tract urinar
inferior (LUTS). Rezultate pe termen scurt
Vasile Dan Stanca, Andrei Boc, Radu Aurel Maxim, Vitalie Gherman, Sergiu Nicolescu, Ioan Coman
87
Analiză cu element nit a unei noi cuști expandabile pentru fuziune intervertebrală
Mihai Magureanu, Dinu Vermesan, Juganaru Iulius, Horia Haragus, Roberta Cecilia Avram, Dan Ioan Stoia,
Gigi Adrian Aiordachioaie
91
Apendicectomia la obezi. Abord clasic sau laparoscopic?
Marius Sfîrlea, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Codru a Macovei, George Dejeu,
Ciprian Borza, Daniela Berdea, Daniela Rahotă
97
Inciden a drenajului limfatic atipic la pacien ii cu melanom malign
Florin Suru, Adrian Maghiar
103
PREZENTARE DE CAZ
Sindromul nefrotic și insu cien a renală acută cauzate de leucemia limfocitară cronică. Prezentare
de caz și o revistă a literaturii
Boris Solun, Dana Marcoviciu, Yulia Belnik, Avraham Sendovski, Dror Dicker, Ana Tovar
109
Litiază vezicală secundară unui dispozitiv intrauterin migrat. Prezentare de caz
Victor Ona, Bogdan Feciche, Andrei Boc, Dan Ona, Ioan Coman
115
MEDICINA ȘI ARTA
Picturile reprezentând un caz de obezitate din secolul al XVII-lea, datorat probabil sindromului
Prader-Willi
Călin Bumbulu , Andrei Bumbulu , Alina Daniela Negru, Rumelia Koren
119
EVENIMENT MEDICAL
Invita ie la Zilele Medicale Sătmărene edi ia a X-a, 4-6 octombrie 2013
122
STANDARDE DE PUBLICARE
123
Colegiul Medicilor
Satu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală,
apolitică şi fără scop patrimonial. Este într-o largă accep iune o organiza ie profesională
liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar
când are ceva important de spus, să nu critice până când nu are solu ii şi să nu propună decât
solu ii rezultate din sfatul colectiv. For a Colegiului Medicilor constă în prezentarea în fa a
societă ii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical
and non-pro t. In a widley acception it is a liberal professional organization and brings
together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to
speak only when he has something important to say, to make no critics until he has solutions
and to propose only solutions resulted from a of collective advice. e force of Physicians
College consist in showing in front of the society an authentic voice, always validated, from
all its members.
Eroilor Revolu iei Pl. no.23, 440055 Satu Mare, Romania.
Tel./Fax: +40-261-710456, +40-361-408164, e-mail: colmedsm@gmail.com
EDITORIAL
THE POWER OF IDEOLOGIES
“- Baby, you still love me?
- I will love you forever my love!”
is banal dialogue is not about love, as it would
was just about the ‘liberalization’ of insurances. We are
seem at rst glance. It is about certainty, the certainty of
going to have several health insurance houses, patients
love in this case. People are hungry for certainty: the
will pay more co-payments, etc. Before any other
certainty of love, health, wealth and eternal life. But
comment I would remind you that in England, Sweden
what fore do we need all these certainties? For having
and Denmark doesn’t exist such ‘freedom’ of choice, but
left the necessary energy and time to do what we want
they have the most e ective healthcare in the world. In
without a care. e a iction of modern society is that
America the freedom is total (you can even not make
the certainties disappear slowly from the world. God
health insurance!) but the system is expensive. So what
died, as atheists found in ancient times, but never had
we want for us? Better health care, fair and
the courage to say it loud until to Nietzsche. Physical
comprehensive, or ideological purity and victory of free
laws of nature have become increasingly complex as to
market in health care?
e purpose of private health
be inaccessible to most mortals. e only certainty is the
insurance companies is to make money and not to
law of universal evolution, that does not bring us peace,
care about sick people! Not the social solidarity and
but the anxiety from which we want to stay away with
mutual aid is their target, but to sell fear. Fear of illness
all our powers. Of course, neither the human nature is
and disability which you have to face alone and for what
changing, but even that does not bring us the peace,
it’s better to tighten your belt to save and give them the
only explains our hunger for certainty. In the absence of
money for management. Fear of re, ood, earthquake
God, hunger for certainty had slaked somehow, and
and malpractice for which we all pay but we do not see
then appeared ideologies. ey deliver your package of
any money, or at best much less than they promised.
certainties, but do not specify the expiration date and
e fact that people live in families and social networks
the major adverse e ects too. In the past century we
which intervene helping a member stricken by a
were infected with fascism, then communism, but
misfortune, is a great handicap for insurers. Or an
unfortunately we remained sensitive to many other
advantage to the extent that people solve their problems
possible future ideologies. In recent years we have
with their friends and give up to claim the rights for
contaminated, at least at the level of elite, by the
which they paid.
ideology of ‘the free market’.
Let’s try to imagine what it will be with more private
Years ago, when I still did sometimes one political
health insurance companies. I ask you that in this
feverish, a young and spirited liberal asked, ‘What do we
process do not forget the premise told above (with bold
have to do to ensure the victory of the free market in
characters). I will start directly with the conclusion: the
healthcare?’ First I did not understand the question:
quality standards of sick care will fall. My argument is
‘What do you mean by victory of the free market? I thought
taken by an experience that we, all he car owners lived.
that, we doctors, we ght against disease and su ering and
In the last year there were several scandals regarding the
not for or against the free market victory or collectivism.’ It
car insurance. Under the pressure of market competition
will not recount the rest of the dialogue because my
and the desire to win, some insurers have agreed service
interlocutor remained deaf and blind to my pragmatic
workshops that used forged parts, more cheaper, instead
arguments, though he had medical training (he did not
of the originals with manufacturer’s warranty. Once
practice because of the exhausting demands of public
word spread, they denied it vehemently, but did not fail
life). But the problem
(the infection) remained and
to provide more expensive insurance for those who
worsened sharply in the recent months with new
wanted the original pieces. Who won? e car owner
proposals to amend the health law in Romania. In fact it
pays more for the fear of counterfeits, the manufacturer
7
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
of original parts produces the same or less and sells
after the introduction of this system, health expenditure
about on the same price, the manufacturer of fake parts
in healthcare increased by 40% in a few years, without
is producing and selling some less, and the auto shop
signi cant increase in satisfaction and quality. My
receives the same money for labor. e only winner is
patients already ask me: ‘Doc, when we begin to pay?’ e
the merchant of fear. I think that the advertising
question has, however, two distinct shades: the elderly,
industry should change its slogan: not the sex sells, but
the unemployed and the poor asks me with concern that
the fear sells better.
e same thing will happen in
they would not allow the regular medical care, the
healthcare? No doubt, and more, the little social
wealthy class eagerly hoping that if they pay they will
solidarity that we had will go down the drain (one
not stand in line with everyone else. Dear fellows, what
chapter that Romanian society stands still bad!). If it we
would you have respond to them? What do we want as
were not blinded by the free market ideology, our
society, because if we want a strong society it would be
reformers should have told us that in the Netherlands,
appropriate not to sit idly and let ideologies to lead us!
Sever-Cristian Oană, MD
8
ORIGINAL ARTICLES
DETECTION OF IgG ANTI LAMININ 1 ANTIBODIES IN PATIENTS
WITH ACUTE ISCHEMIC STROKE
Manole Cojocaru1, Elena Rusu2, Inimioara Mihaela Cojocaru3, Isabela Siloşi4
1Department of Physiology, Faculty of Medicine, Titu Maiorescu University, Bucharest, Romania, 2Department of
Biochemistry, Faculty of Dental Medicine, Titu Maiorescu University, Bucharest, Romania, 3Department of Neurology,
Carol Davila University of Medicine and Pharmacy, Bucharest, Romania, 4Department of Immunogy, Faculty of
Medicine, University of Medicine and Pharmacy, Craiova, Romania
Address for correspondence:
Cojocaru Manole
5 omas Masaryk St., Sector 2, Postal Code 020983, Bucharest, Romania
Email: mancojocaru@yahoo.com
Received: 17.02.2014
Accepted: 28.02.2014
Med Con March 2014 Vol 9, No 1, 9-11
Abstract
signi cantly with the clinical outcome (157.16±13.82
IU/mL; p<0.009). ALA is not disease speci c, but seem
Background: e presence of IgG anti-laminin-1
to be associated with lupus anticoagulant
(LA),
antibodies
(ALA) may de ne a subset of primary
anticardiolipin antibodies (aCL). e negative predictive
antiphospholipid syndrome (APS) patients at greater
value of IgG ALA was 84%, and positive predictive
risk for thrombosis.
value of IgG ALA was 75%.
Objectives: To analyzed the prevalence of IgG ALA
Conclusion:
e results con rm that these
in blood samples from patients with acute ischemic
autoantibodies are released into the blood after the
stroke and to assess whether these antibodies are
stroke, they can be easily measured, and they correlate
associated with clinical outcome.
with the outcome. Higher peak serum levels of IgG
Materials and methods: e study included 78
ALA correlated well with worse clinical outcome. e
patients with acute ischemic stroke, 46 females and 32
presence of IgG ALA seems to re ect an alteration of the
males, ranges from 46 to 81 years, mean age 74.3±6.8
blood-brain barrier that promotes the access of central
years. Blood samples for IgG ALA measurement were
nervous system antigens to immunocompetent cells.
taken within 24 hours after the onset of the ischemic
Keywords: anti-laminin antibodies, prevalence,
stroke and in 72 healthy controls 43 females and 29
clinical outcome, acute ischemic stroke
males, ranges from 42 to 79 years, mean age 71.3±6.4
years. Serum IgG ALA were measured by means of
Introduction
ELISA. For statistical analysis, we used the Fisher’s exact
test, odds ratio, and 95% con dence interval (CI) in
In ammation and oxidative stress are important
each case. A value of p<0.05 was considered signi cant.
factors that contribute to disruption of the blood-brain
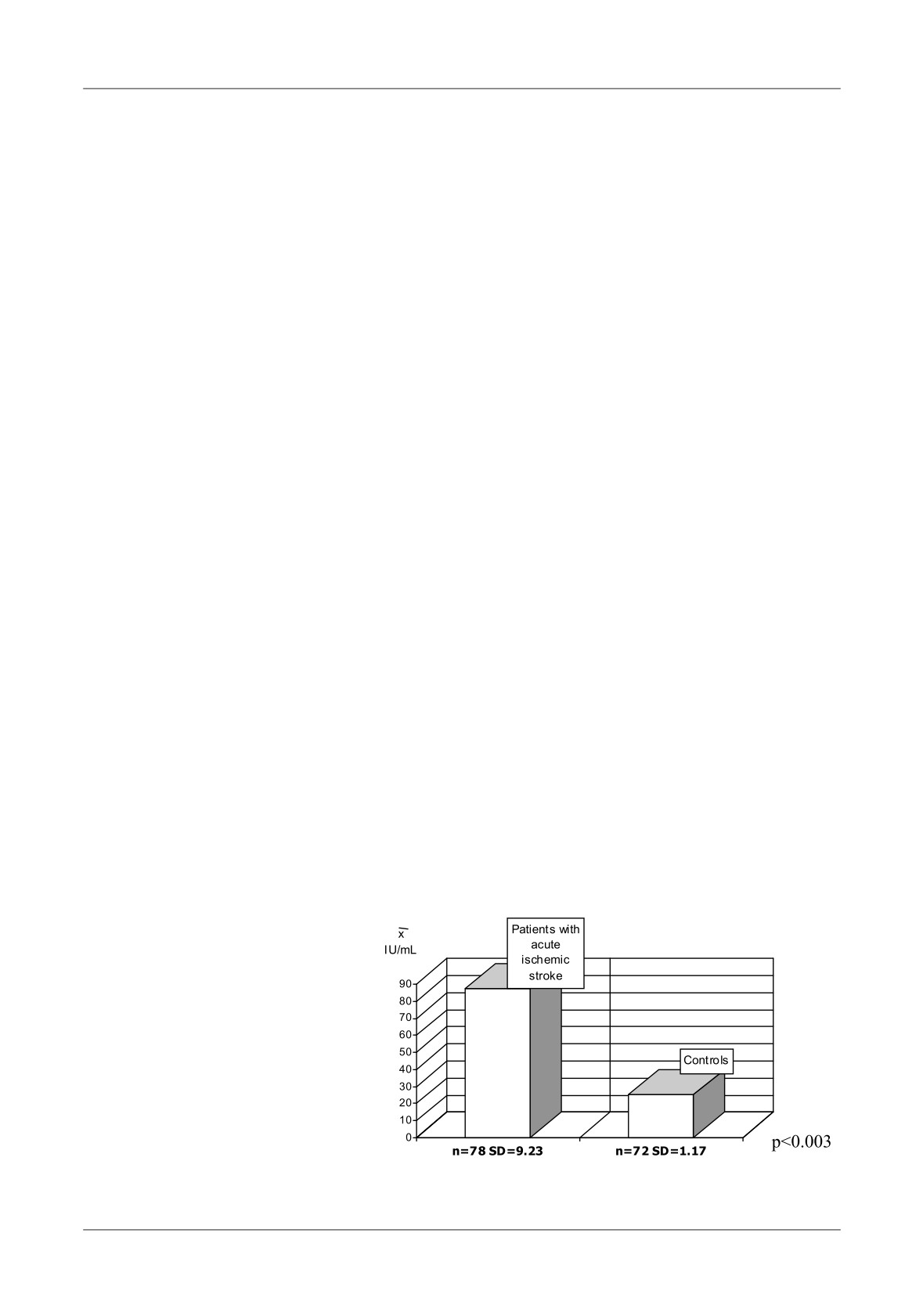
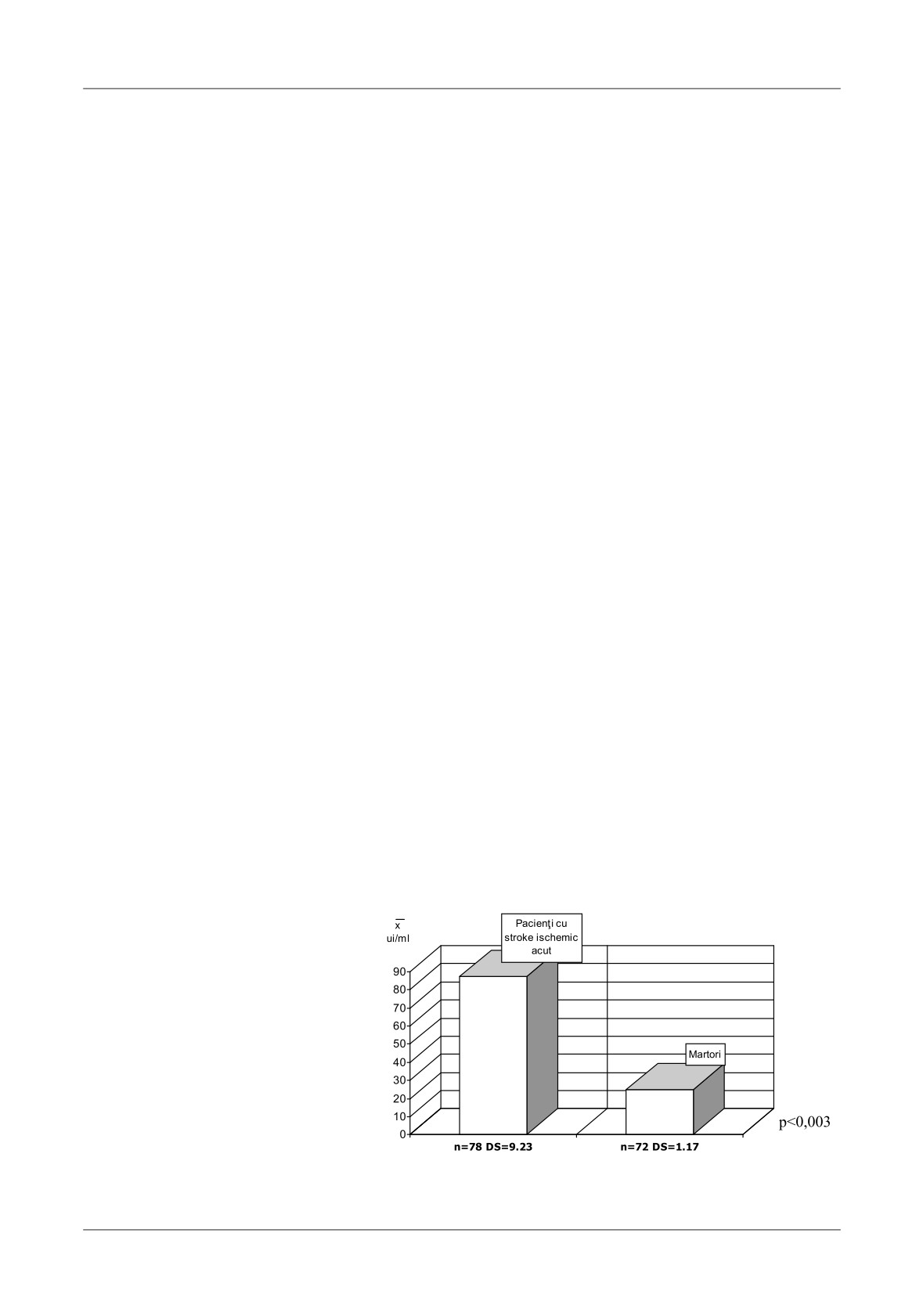
Results: High titers of serum IgG ALA were
barrier (BBB) [1]. Mechanisms include disruption of
detected in 58 (76%) patients. e IgG ALA titers in
inter-endothelial
tight-junction complexes and
patients with ischemic stroke were signi cantly higher
induction of proteases, in particular matrix
(127.32±13.42 IU/mL) than in the controls
metalloproteinases
(MMPs), which
degrade
(26.41±1.83 IU/mL) (p<0.003).
e titer correlated
constituents of the vascular basement membrane [2].
Detection of IgG Anti-Laminin-1 Antibodies in Patients with Acute Ischemic Stroke
9
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Breakdown of BBB is an important contributing factor
e relationship between the prevalence of IgG
to injury in many brain diseases, including stroke [3-5].
ALA and clinical outcome were analyzed by the Fisher’s
Laminin-1 is a multifunctional glycoprotein of the
exact test. A value of p<0.05 was considered statistically
basement membrane. e ability to maintain BBB
signi cant.
e Pearson’s correlation coe cient test was
integrity depends on adequate structural support from
used to assess the correlation between the IgG ALA
the basement membrane.
e antibodies might be
titers to the clinical outcome.
clinically important in the development of ischemic
e local ethics committee approved the clinical
stroke [6-8].
protocols, and all patients, including controls, provided
e objective of this study was to analyzed the
informed consent.
prevalence of IgG ALA in blood samples from patients
with acute ischemic stroke and to assess whether these
Results
antibodies are associated with clinical outcome.
Signi cantly high titers of IgG ALA antibodies were
Material and Methods
observed in
58 (76%) patients with acute ischemic
stroke compared to controls.
e IgG ALA titers in
Serum titers of IgG ALA immediately after
patients with acute ischemic stroke were signi cantly
admission for acute ischemic stroke in 78 patients (46
higher (ranges from 94.16 to 156.07 IU/mL, mean
females and 32 males, ranges from 46 to 81 years, mean
value 127.32±13.42 IU/mL) than in controls (ranges
age 74.3±6.8 years), and in 72 healthy controls (43
from 16.08 to 31.67 IU/mL, mean value 26.41±1.83
females and 29 males, ranges from 42 to 79 years, mean
IU/mL) (p<0.003).
e titer correlated signi cantly
age 71.3±6.4 years) were measured.
with the clinical outcome
(ranges from
134.03 to
Patients with a history of atrial brillation, valvular
188.02 IU/mL, mean value
157.16±13.82 IU/mL;
heart disese,
(as shown on echocardiography), or
p<0.009). Peak plasma levels of IgG ALA correlated
connective tissue disease were excluded from the study,
well with injury severity and outcome in the rst 24
as were those with a previously undetected cardiac
hours after the onset of the ischemic stroke.
source of thrombus. Also, exclusion criteria were: severe
A signi cant statistical correlation between IgG
medical or psychiatric illness,
in ammatory
ALA titers and GCS (r=0.79, p<0.009) and a signi cant
gastrointestinal disease, serum creatinine >150mmol/L,
statistical correlation between IgG ALA levels of NIHSS
gout or renal failure or took of antioxidant vitamins,
groups
(16-42 points-bad prognosis,
7-15 points-
iron de ciency.
intermediate prognosis, and 0-6 points-good prognosis)
TOAST and OCSP criteria, National Institutes of
were observed (r=081, p<0.005).
Health Stroke Scale (NIHSS) and Glasgow Coma Score
e negative predictive value of IgG ALA was 84%,
(GCS) at baseline and at 24 hours were used. Cerebral
and positive predictive value of IgG ALA was 75%.
ischemia was documented by an imaging technique.
Patients with IgG ALA in serum demonstrated
Ultrasound examination of cervico-cerebral arteries
serious thrombotic manifestations.
and of heart was performed.
A sample (5mL) was taken within
24 hours after the onset of the
ischemic stroke by vein puncture. e
serum was separated by centrifugation
at 4000g for 5 min and stored as 0.5
mL aliquots at -200C until an ELISA
was performed.
e results were expressed as
arbitrary units (IU/mL). ROC curve
was used to calculate the cut o value.
Mean values (x) ± standard deviation
(SD) were used. We used the Fisher’s
exact test, odds ratio, and
95%
con dence interval (CI) in each case.
Titers of IgG ALA were compared by
Figure 1. Mean value of IgG anti-laminin-1 antibody titers in patients
the Student t test.
with acute ischemic stroke as compared to controls
10
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Discussion
References
e association between the IgG ALA and
1.
Adams HP, Adams R, del Zoppo G, Goldstein LB.
ischemic stroke was analyzed in 78 positive patients.
Guidelines for the early management of patients with
e presence of the autoantibodies signi cantly
ischemic stroke:
2005 guidelines update. Stroke
correlated with ischemic stroke. We demonstrated that
2005;36(4): 916-21.
patients with acute ischemic stroke had signi cantly
2.
Maas MB, Furie KL. Molecular biomarkers in stroke
higher levels of IgG ALA. Our ndings suggest that
diagnosis and prognosis. Biomark Med 2009;3(4): 363-83.
IgG ALA may have a harmful e ect on events at early
3.
Doyle KP, Simon RP, Stenzel-Poore MP. Mechanisms
stages of ischemic stroke. Our observations suggest
of ischemic brain damage. Neuropharmacology
that IgG ALA may be responsible for ischemic stroke,
2008;55(3):310-18.
interfering with the in ammation. Anti-laminin-1
4.
Laterza OF, Modur VR, Crimmins DL, et al.
antibodies are not disease speci c, but seem to be
Identi cation of novel brain biomarkers. Clin Chem
associated
with
lupus
anticoagulant
(LA),
2006;52(9):1713-21.
anticardiolipin antibodies
(aCL)
[5]. Laminin, a
5.
Sotgiu S, Zanda B, Marchetti B, et al. In ammatory
multifunctional glycoprotein of basement membranes,
biomarkers in blood of patients with acute brain
consists of three di erent subunits, a, b and g chains.
ischemia. Eur J Neurol 2006;13(5):505-13.
To date, at least 15 isoforms of laminin are known.
6.
Broughton BR, Reutens DC, Sobey CG. Apoptotic
Laminins are involved in diverse biological activities,
mechanisms after cerebral ischemia. Stroke 2009;40(5):
including the promotion of cell adhesion, migration,
e331-e339.
proliferation and di erentiation, as well as the
7.
Hill MD. Diagnostic biomarkers for stroke: a stroke
formation of the sca olding network in basement
neurologist’s perspective. Clin. Chem 2005;51(11):2001-2.
membranes [6,9].
8.
Whiteley W, Tseng MC, Sandercock P. Blood
ese biological processes occur through signal
biomarkers in the diagnosis of ischemic stroke: a
transduction and cell-matrix interactions mediated by
systematic review. Stroke 2008;39(10):2902-9.
laminin-speci c receptors and other matrix components.
9.
Bornstein NM, Aronovich B, Korczyn AD, Shavit S,
Many of the responsible sites for these activities are
Michaelson DM, Chapman J. Antibodies to brain
localized in the carboxyl-terminal globular G domain of
antigens following stroke. Neurology 2001;56(4):529-30.
the a chain [10-13].
10.
Zierath D, ullbery M, Hadwin J, Gee JM, Savos A,
e presence of IgG ALA may de ne a subset of
Kalil A, Becker KJ. CNS immune responses following
patients at greater risk for worse outcome. In light of
experimental stroke. Neurocrit Care 2010;12(2):274-84.
these ndings, the assessment of IgG ALA might prove
11.
Colognato H, Yurchenco PD. Form and function: the
useful for the clinical management of patients with
laminin family of heterotrimers. Dev. Dyn
acute ischemic stroke. IgG ALA could be a useful
2000;218(2):213-34.
serologic marker in patients with various thrombotic
12.
Denes A,
ornton P, Rothwell NJ, Allan SM.
manifestations [14].
In ammation and brain injury: acute cerebral
Conclusion
ischaemia, peripheral and central in ammation. Brain
e present study assessed the clinical signi cance
Behav Immun 2010;24(5):708-23.
of IgG ALA. Our clinical study showed that high levels
13.
Ruleva NIu, Kuzin VM, Martynov MIu, Kamchatnov
of IgG ALA in the blood are signi cantly associated
PR. Markers of in ammation, autoantibodies to
with the ischemic stroke. Patients with high titers of
neurospeci c antigens and outcome in patients with
IgG ALA are at higher risk of developing thrombotic
acute ischemic stroke. Zh Nevrol Psikhiatr Im S S
events. IgG ALA could be a useful serologic marker in
Korsakova 2004;(Suppl 12):60-5.
the early treatment in patients with thrombotic
14.
Aumailley M, Pesch M, Tunggal L, Gaill F, Fassler R.
manifestations. Signi cant statistical correlations
Altered synthesis of laminin 1 and absence of basement
between IgG ALA titers and clinical outcome were
membrane component deposition in b1 integrin-de cient
observed (NIHSS and GCS score).
embryoid bodies. J Cell Sci 2000;113Pt2:259-68.
Detection of IgG Anti-Laminin-1 Antibodies in Patients with Acute Ischemic Stroke
11
ORIGINAL ARTICLES
THE ASSOCIATION OF ORAL LICHEN PLANUS WITH CHRONIC
HEPATITIS C. RETROSPECTIVE STUDY
Carmen Gheorghe1, Lelia Mihai2, Ioanina Parlatescu1, Şerban ovaru1, Elena Coculescu1
1Discipline of Oral Pathology, Faculty of Dentistry, University of Medicine and Pharmacy Carol Davila, Bucharest,
2Discipline of Oral Medicine, University of Medicine Titu Maiorescu, Bucharest
Address for correspondence:
Carmen Larisa Gheorghe
Bucureşti, 4-5 Eforie St, 3rd Floor, 18th Room
Phone: 0749218099
E-mail: larisacarmen74@gmail.com
Received: 18.02.2014
Accepted: 28.02.2014
Med Con March 2014, Vol 9, No 1, 13-17
Abstract
lichen planus in patients who associated hepatitis C
infection was in 44% of cases the erosive one.
Oral lichen planus is a dermatologic condition quite
Conclusions: e results showed an association of
common in current dental practice. e association of
hepatitis C more frequent in patients with oral lichen
lichen with chronic hepatitis C has been observed,
planus. ese data highlight the need to achieve hepatitis
lichen planus being thus considered one of the
C screening of all patients diagnosed with oral lichen
extrahepatic manifestations of hepatitis C virus
planus. Erosive, acute lichen planus appears to be
infection. In these cases the clinical appearance of lichen
characteristic of patients associated liver pathology.
planus is more aggressive, with acute symptoms and its
Keywords: oral lichen planus
, hepatitis C,
evolution presents more frequent exacerbation periods.
extrahepatic manifestations , erosive form
e purpose of this study is to analyze the possibility of
associating oral lichen planus with chronic hepatitis C
Introduction
and to investigate whether there are some clinical forms
of oral lichen planus characteristic for this association.
Oral lichen planus
(OLP) is a chronic, non-
Methods: We performed a retrospective study
in ammatory disease, with severe mucocutaneous
analyzing the medical charts of 380 patients diagnosed
involvement. Clinical lesions mostly common a ect
with oral lichen planus in the clinical service of the
the malpighian epithelium of the skin and oral mucosa,
Department of Oral Pathology, University of Medicine
the esophageal mucosa, genital or scalp [1,2]. In rare
and Pharmacy Carol Davila, Bucharest between 2007-
cases, lesions can appear also on the nails. In such cases
2010.
ese patients were investigated with serological
the complications may be the irreversible destruction of
tests for hepatitis C markers and the clinical form of oral
the nail matrix (or the root of the nail), nail thinning or
lesions at the time of presentation.
loss [1]. OLP prevalence in the general population is
Results: From the selected patients 18% (50/273)
variable, recent studies reporting values of 0.5-2.5 %
presented a concomitant infection with hepatitis C,
[3]. Adult women are a ected with preference in 5-6
signi cantly higher compared with patients in the
decades of life, and only in exceptional children [3,4].
control group 6% (8/143). e main clinical form of
Etiopathogenesis of OLP is today a subject of intense
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
13
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
discussion. It is considered that immunological
mucosa. From the laboratory investigations of the
reactions act an important role in triggering the
charts, it has been investigated the determination of
pathophysiological mechanism. e modi ed antigens
HCV-Ab by ELISA II-III generation. In case of positive
stimulate basal cells and Langerhans cells thereby
results have been recommended con rmatory testing,
triggering a cascade of immunological reactions that
immunoblot method, which determines speci c IgG
ultimately will determine the basal keratinocyte
antibodies anti-HCV.
apoptosis
[4,5].
e oral lesions often have typical
us was formed the study group which consists of
clinical appearance and location. Typically OLP
273 patients diagnosed with OLP. OLP diagnosis was
presents keratotic lesions, atrophic, erosive or rare
established on clinical criteria mainly being considered
bullous lesions [6].
e associated symptomatology is
only cases with typical clinical appearance and
related by patients, especially in serious cases, with
characteristic location of the lesions. Histologic
predominating atrophic or erosive lesions. e dynamic
con rmation of the clinical diagnosis was made in 205
and temporal variability of clinical lesions are largely
cases
(75%) who had no changes in hematological
in uenced by age and level of activity of the disease
laboratory
constants
and had no general
[2,4].
e evolution of lichen planus is chronic during
contraindication for biopsy. As a complementary
the succeeding periods of exacerbation of oral lesions
diagnostic investigation in 2 cases was performed the
with periods of remission in which symptoms are
direct immuno uorescence, and in
3 cases the
reduced. Unlike cutaneous forms, OLP has a much
immunohistochemistry examination.
longer trend, over many years and can have an
e control group consisted of 143 patients without
unsatisfactory therapeutic response in some cases [4].
alterations or lesions of the oral mucosa in the
As the association with chronic liver disease , especially
examinations which were presented in our service
chronic hepatitis C is a well-documented issue, there is
perception disorders of the oral mucosa without
also the hypothesis that hepatitis C virus ( HCV) may
corresponding clinical symptoms suggestive of the
be involved in the pathogenesis of OLP [7,8,9].
e
diagnosis of burning mouth syndrome. Patients in the
mechanisms involving in the pathogenesis of HCV are
control group were tracked data on age and gender and
currently lichen planus explained through HCV
the results of this analysis for determining HCV-Ab.
replication being present, not only in hepatocytes but
also in extra hepatic cells, causing their damage due to
Results
lysis and cytopathic e ect
[10].
e study aims to
investigate the possibility of OLP association with
e study group consisted of 273 patients aged
chronic hepatitis C and review clinical forms that these
between 20 and 95 years (mean age 56.87). Of these,
patients presented during the examination.
219 patients (80%) were women and 54 (20%) men.
Regarding family history, 5 patients reported that
Material and methods
relatives had medical history of cutaneous and oral
lichen planus, one patient had a family history of lupus
A retrospective study was conducted by analyzing
and eight patients had cases of carcinomas of the
the data from the medical charts of 380 consecutive
digestive tract or oral cavity.
patients clinically diagnosed with OLP in the service of
A total of 156 (57%) patients stated that the onset
the Department of Oral Pathology, University of
of OLP coincided with a severe emotional stress, 89
Medicine and Pharmacy Carol Davila, Bucharest
(33%) patients denied this association and 28 (10%)
between 2007-2010.
patients could not specify whether they had noticed a
Criteria for inclusion in the study were represented:
link causal e ect between the two aspects. Regarding
analytical study design, patients diagnosed with OLP,
the time interval from referral oral lesions, it had variable
tests for determining anti -hepatitis C virus (HCV-Ab).
values.
us, 71 (26%) patients were presented at the
From the medical charts of the selected patients for
rst consultation in less than three months from the
this study were extracted general information regarding
onset of complaints,
45
(16%) patients after
3-6
the gender, age and background of the patients, a
months, 52 (19%) patients were diagnosed with OLP
medical family history and personal pathological data,
after about 1 year of onset, 58 (21%) patients after 1-5
presentation reasons, symptoms and the time of onset.
years, and 23 (8%) of patients complain of symptoms
ere were also tracked references to chronic stress
present for more than 5 years. In 9% of cases (24
associated with disease onset at the time of clinical
patients) could not be determined accurately the onset,
appearance and the number of a ected areas of the
patients were not able to clarify this issue.
14
Gheorghe et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Following determinations HCV-Ab in the study
group, 50 (18%) patients had positive results, and 223
(82%) patients had negative results (Figure 1).
In the subgroup analysis the distribution of some
variables was studied: age, sex, symptoms accused, the
clinical presentation and the number of areas involved
in patients with OLP associating HCV.
us were
obtained the following results: the group of the
50
patients who were diagnosed with HCV infection
concomitant with OLP was composed of 46 (92%)
women and 4 men (8%). About the age, it was in the
range 41-83 years, with a mean age of 63 years. Clinical
types seen in patients with hepatitis C are predominantly
Figure 1.
e results show the presence
erosive form in 22 (44%) cases, followed in order of
of statistically signi
cant HCV-Ab in the study group
frequency of keratotic forms in
18 (36%) cases of
atrophic forms in 8 (16%) cases and only two (4%)
cases of bullous predominant forms. According to the
severity of the clinical symptomatology of patients had
varying degrees of intensity, but the symptoms were
present in
45 (90%) patients, while only
5 (10%)
patients were asymptomatic. Regarding the location of
the clinical lesions in patients who have associated
chronic hepatitis C, acute forms predominated,
involving large, over 4 areas in 27 (54%) cases. Oral
lesions a ected the bilateral buccal mucosa 10 (20%)
patients, the three involved areas 3 have been found in
11 (22%) cases, while unilateral lesions were observed
only in 2 (4%) patients.
Analyzing the structure of the control group in this
Figure 2. Patients in the control group had
study, it was noted that about the gender distribution of
a lower risk of being infected with HCV
patients 98 (69%) patients were female and 45 (31%)
men and the average age was calculated from value of
55.95. After analyzing the results obtained from the
Table I. e erosive form of OLP was observed most
determination of HCV-Ab was observed that
135
frequently in patients with associated chronic hepatitis C
(94%) were negative and 8 (6%) were seropositive
Clinical form
No of cases
Percentage
(Figure 2).
Erosive
22
44%
Comparing results, it is observed that patients
diagnosed with OLP in the study group had a
Keratotic
18
36%
signi cantly higher risk of infection associated with
Atrophic
8
16%
HCV (50/273, 18%) than patients in the control group
Bullous
2
4%
(8/143, 6%). Regarding the clinical, erosive lesions are
prevalent in patients diagnosed with oral lichen planus
presenting as hepatitis C associated pathology (Table I).
incidence of extrahepatic autoimmune manifestations
in patients with chronic HCV infection.
Discussions
e results obtained in clinical trials addressing this
issue have been contradictory, being largely dependent
Correlation between OLP and chronic liver disease,
on the area in which they were made and less than age
especially chronic HCV hepatitis was rst observed in
or sex of the patients.
is is explained by the variable
1978 by Rebora, and since then numerous studies have
incidence of HCV infection on Earth , there are areas
been conducted on this topic. e particularity of HCV
which show a low endemic risk
(North America,
to infect both liver cell and lymphocyte gives its
Northern Europe), medium risk endemic (South and
ubiquitous nature, the consequence being a higher
South-East Europe South America, Central America,
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
15
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Australia, Central and Eastern Europe Sub-Saharan
association OLP and chronic HCV infection and some
Africa, South Asia) or high (North Africa, Middle East,
form of oral disease clinic [14].
Central Asia and Eastern Europe) [11].
Our study presented 273 patients diagnosed with
Conclusions
OLP which were determined HCV-Ab and clinical
description of the lesions present at the moment of rst
It is recommended a careful follow-up of patients
clinical exam.
e results showed a signi cantly higher
with OLP who associate HCV infection because it has
seropositivity for hepatitis C markers in patients
been known that in this situation the evolution presents
included in the study group compared with the control
periods of exacerbation of clinical lesions if the
group. Also, the predominant clinical form was the
decompensation of liver disease appears.
erosive type in patients chronically infected with HCV
Tracking the status of liver function is important
and symptoms were present most cases.
because it associates the worsening of hepatitis and the
Studies from medical literature shows similar results
relapse of lichen planus.
as our study in Spain, Italy and Japan, countries that
Most times patients who associate OLP and acute
pose a risk for HCV infection endemic environment,
HCV infection have erosive forms accompanied by
like as our country.
us Carrozzo et al., making a
signi cant symptoms that cause functional disorders
prospective study on a sample of 70 patients diagnosed
a ecting the patient and his personal life.
with oral lichen planus and a control group of
70
Survey results show that hepatitis C can be involved
patients all concordant for age and sex with the study
in the pathogenesis of oral lichen planus.
group noted a higher prevalence of HCV infection in
is proves the importance of screening for the
the study group than in controls [12]. A clinical study
presence HCV-Ab in patients diagnosed with OLP.
led by Lodi in Italy in
2004, which included 581
Acknowledgement:
is paper is supported by the
patients, 303 in the study group and 278 in the control
Sectoral Operational Programme Human Resources
group obtained the following results: 19.1% of patients
Development (SOP HRD) 2007-2013, nanced from the
with oral lichen planus presented and Ac anti- HCV
European Social Fund and the Romanian Government
positive, while in the control group the percentage of
under the contact number POSDRU/107/1.5/S/82839.
patients with HCV-Ab present was only 3.2% [13].
A similar study conducted in the population of
Israel showed comparable results [14].
In research achievements in Spain, Bagan et al have
References
investigated a group of 100 patients diagnosed with
OLP which were determined HCV-Ab and found in
1. Eisen D. e evaluation of cutaneous, genital, scalp,
23% of cases positive results.
e control group was
nail, esophageal and ocularinvolviment in patients with
composed of 100 patients clinically healthy all without
oral lichen planus. Oral Surg Oral Med Oral Pathol
lesions suggestive of OLP, only
5% of HCV-Ab
Oral Radiol Endod 1999;88(4):431-6.
determinations were present.
e prevalence of HCV
2. Scully C, Carozzo M. Oral mucosal disease: Lichen
infection in patients with OLP was higher in the study
planus. Br J Oral Maxillofac Surg 2008;46(1):15-21.
group than in the control group. ese results warrant
3. McCartan BE, Healy CM. e reported prevalence of
investigation of potential HCV infection in patients
oral lichen planus; a review and critique. J Oral Pathol
with OLP [15].
Med 2008;37(8):447-53.
At the opposite pole are the results of studies in
4. Tovaru S, Tovaru M, Costache M, Demarossi F.
England which found no link between the two disorders
Medicină şi patologie orală. Vol I. Q Med Publishing,
[16].
2008.
Regarding clinical form, some studies show similar
5. Sugerman PB, Savage NW, Walsh LJ, et al. e
results of our study.
us Carrozzo et al. found in the
pathogenesis of oral lichen planus. Crit Rev Oral Biol
lot of patients with associated chronic HCV infection
Med 2002;13(4):350-65.
58.8% the erosive form of OLP [12]. All erosive forms
6. Crispian Scully. Oral and Maxillofacial Medicine. e
of OLP were observed in another study conducted in
Basis of Diagnosis and Treatment. Second edition,
Italy
[17], while other authors have found that the
Churchill Livingstone Elsevier, 2008.
predominant clinical form reticular form [18].
7. Gheorghe C, Mihai L, Parlatescu I, Tovaru S. Afec iuni
On the other hand, in the study conducted in the
ale mucoasei orale asociate cu infec ia cu virus hepatitic
population of Israel found no correlation between the
C: lichenul plan bucal. Med Con 2013;41(8):101-104.
16
Gheorghe et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
8. Lodi G, Pellicano R, Carrozzo M. Hepatitis C virus
and a systematic review. Br J Dermatol 2004;151:1172-
infection and lichen planus: a systematic review with
81.
meta-analysis. Oral Dis 2010;16(7):601-12.
14.
Yarom N, Dagon N, Shinar E, Gorsky M. Association
9. Lodi G, Giuliani M, Majorana A, Sardella A, Bez C,
between hepatitis C virus infection and oral lichen
Demarosi F, Carrassi A. Lichen planus and hepatitis C
planus in Israeli patients. Isr Med Assoc J
virus: a multicentre study of patients with oral lesions and a
2007;9(5):370-2.
systematic review. Br J Dermatol 2004;151(6):1172-81.
15.
Bagán JV, Ramón C, González L, Diago M, Milián
10. Prabhu S, Pavithran K, Sobhanadevi G. Lichen planus
MA, Cors R, Lloria E, Cardona F, Jiménez Y.
and hepatitis c virus (HCV)-is there an association? A
Preliminary investigation of the association of oral lichen
serological study of
65 cases. Indian J Dermatol
planus and hepatitis C. Oral Surg Oral Med Oral
Venereol Leprol 2002; 68(5):273-4.
Pathol Oral Radiol Endod 1998;85(5):532-6.
11. Mohd Hana ah K, Groeger J, Flaxman AD, Wiersma
16.
Ingafou M, Porter SR, Scully C, Teo CG. No evidence
ST. Global epidemiology of hepatitis C virus infection:
of HCV infection or liver disease in British patients with
New estimates of age-speci c antibody to HCV
oral lichen planus. Int J Oral Maxillofac Surg
seroprevalence. Hepatology 2012; Nov 21.
1998;27(1):65-6.
12. Carrozzo M, Gandolfo S, Carbone M, Colombatto P,
17.
Gandolfo S, Carbone M, Carrozzo M, Gallo V. Oral
Broccoletti R, Garzino-Demo P, Ghisetti V. Hepatitis
lichen planus and hepatitis C virus (HCV) infection: is
C virus infection in Italian patients with oral lichen
there a relationship? A report of 10 cases. J Oral Pathol
planus: a prospective case-control study. J Oral Pathol
Med 1994;23(3):119-22.
Med 1996;25(10):527-33.
18.
Mignogna MD, Lo Muzio L, Lo Russo L, Fedele S,
13. Lodi G, Giuliani M, Majorana A, Sardella A, Bez C,
Ruoppo E, Bucci E. Oral lichen planus: di erent
Demarosi F, Carrassi A: Lichen planus and hepatitis C
clinical features in HCV-positive and HCV-negative
virus: a multicentre study of patients with oral lesions
patients. Int J Dermatol 2000;39(2):134-9.
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
17
Medical Connections/Conexiuni Medicale
Conflict-of-Interest Statement
Medical Connections/Conexiuni Medicale (Med Con) requires all authors and reviewers to declare any
con icts of interest that may be inherent in their submissions.
Con ict of interest for a given manuscript exists when a participant in the peer review and publication
process-author, reviewer, or editor - has ties to activities that could inappropriately in uence his or her
judgment, whether or not judgment is in fact a ected.
Financial relationships with industry, for example, through employment, consultancies, stock
ownership, honoraria, expert testimony, either directly or through immediate family, are usually considered
to be the most important con icts of interest. However, con icts can occur for other reasons, such as
personal relationships, academic competition, and intellectual passion.
Public trust in the peer review process and the credibility of published articles depend in part on how
well con ict of interest is handled during writing, peer review, and editorial decision making. Bias can
often be identi ed and eliminated by careful attention to the scienti c methods and conclusions of the
work. Financial relationships and their e ects are less easily detected than other con icts of interest.
Participants in peer review and publication should disclose their con icting interests, and the information
should be made available so that others can judge their e ects for themselves.
Authors: When they submit a manuscript, whether an article or a letter, authors are responsible for
recognizing and disclosing nancial and other con icts of interest that might bias their work. ey should
acknowledge in the manuscript all nancial support for the work and other nancial or personal
connections to the work.
Reviewers: External peer reviewers should disclose to editors any con icts of interest that could bias
their opinions of the manuscript, and they should disqualify themselves from reviewing speci c
manuscripts if they believe it appropriate. e editors must be made aware of reviewers’ con icts of interest
to interpret the reviews and judge for themselves whether the reviewer should be disquali ed. Reviewers
should not use knowledge of the work, before its publication, to further their own interests.
Manuscript Title: ___________________________________________________________
I declare no con ict of interest
I declare the following potential con ict of interest:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Name
Signature/Date
Please fax or mail this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
Mail: colmedsm@gmail.com
ORIGINAL ARTICLES
CLINICAL AND TOMOGRAPHIC ASPECTS OF ACUTE PANCREATITIS
COMPLICATIONS
Gheorghe Nicolae Sârbu1, Lorant Kiss1, Alina Bereanu1, Roland Kiss1, Dan Maniu2
11st Surgical Clinic,
2Department of Radiology, Academic Emergency Hospital of Sibiu a liated to Lucian Blaga
University, Sibiu
Address for correspondence:
Sârbu Gheorghe Nicolae
Academic Emergency Hospital of Sibiu
2-4 Corneliu Coposu Blvd, PO 550245, Romania, Sibiu
E-mail: dr.sarbu@yahoo.de
Received: 30.01.2014
Accepted: 27.02.2014
Med Con March 2014, Vol 9, No 1, 19-26
Abstract
Introduction
e severity of acute pancreatitis is classi ed into
Most episodes of acute pancreatitis (AP) are mild
ve grades (0-4) using unenhanced CT scan while the
and self-limiting, needing only brief hospitalization.
degree of necrosis is measured by contrast - enhanced
However 20% of patients develop severe disease with
CT scan. Acute pancreatitis
(AP) is sometimes
local and extra pancreatic complications characterized
accompanied by pancreatic necroses, which are
by early development and persistence of hypovolemia
responsible for about 50% of death cases in the early
and multiple organ dysfunctions [1].
phase.
Pancreatic necrosis is the most severe local
Early computerized tomography (CT) severity score
complication because it is frequently associated with
correlates well with the occurrence of complications,
pancreatic infections.
e incidence of the mortality
sepsis and mortality rate.
rate in sterile and infected necrosis is 10% and 25%
e advantage of intravenous contrast-enhanced
respectively.
e severity of acute pancreatitis is classi ed
CT imaging in staging acute pancreatitis is based on its
into ve grades (0-4). An unenhanced CT scan and the
capacity to directly assess the morphology of the gland
degree of necrosis are measured by contrast- enhanced
and the involvement of the retroperitoneal peripancreatic
CT scan [2].
tissues.
Complications that occur during an episode of
e extent of the necrosis of the pancreatic gland
pancreatitis are responsible for 2% to 10% mortality
can be quanti ed into below 30 % up to 50 % or over
rates reported in this disease [3,4,5,6].
50 % and the general accuracy of CT in highlighting
Early systemic complications associated with
the necrosis, surgically con rmed was over 87%.
Multisystem Organ Failure or multiple organ failure
e management of patients with acute pancreatitis
(MSOF), are responsible for
20% to 50% of the
is based on the early assessment of severity of the
mortality rate reported with acute pancreatitis [7,8,9].
disease.
e rst
2-3 days are the early complications, with
Keywords: acute pancreatitis, early complications,
clinical manifestations belonging to the cardio-vascular,
late complications
pulmonary, renal and metabolic systems.
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
19
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
e intermediate
2-5 weeks, re ect the
e inclusion criteria for AP and severe forms were
manifestations of the local, retroperitoneal infections,
de ned as: severe pain, the symptoms of acute
infected necrosis, abscess, pseudo cysts, gastrointestinal
respiratory distress syndrome (ARDS), at least 3 fold
and biliary complications.
e late period, months-
elevated serum amylase levels, positive CT with intra or
years, is the time for vascular and hemorrhagic
extra pancreatic disorders, C-reactive protein (CRP) of
complications, pancreatic ascites.
>60 to >250 mg/L, renal failure with creatinine >180
e purpose of this study was to present a diagnostic
µmol\L.
strategy and therapeutic conduct adapted to the severity
In the early stage the clinical presentation and the
of each case.
extent of systemic failure were correlated with cardiac
complications, pulmonary, kidney and metabolic
Materials and Methods
changes.
For intermediate complications, the controlled
A total of 103 patients (60 male and 43 female)
elements were infected pancreatic necrosis, with local
with predicted severe AP were enrolled from March
and systemic complications, gastrointestinal and biliary
2002-March 2012 in the Department of 1st Surgical
complications, and solid organ involvement.
Clinic of Sibiu Academic Emergency Hospital.
As for the late complications were examined vascular,
e etiology of pancreatitis was metabolic
hemorrhagic complications and pancreas ascites.
(alcoholism) in
41 cases
(31 male and 10 female),
mechanical, 46 cases (22 male and 24 female), vascular
Results
in 5 cases (3 male and 2 female), infectious in 11 cases
(4 male and 7 female).
Early systemic manifestations with systemic
e clinical expression and the content of systemic
complications were detectable: pulmonary in ltrate /
failure di er from case to case, in correlation with the
pleural e usion (41 patients), ARDS (acute respiratory
severity of the disease in early stages.
distress syndrome) (21 patients), oliguria
(82 cases),
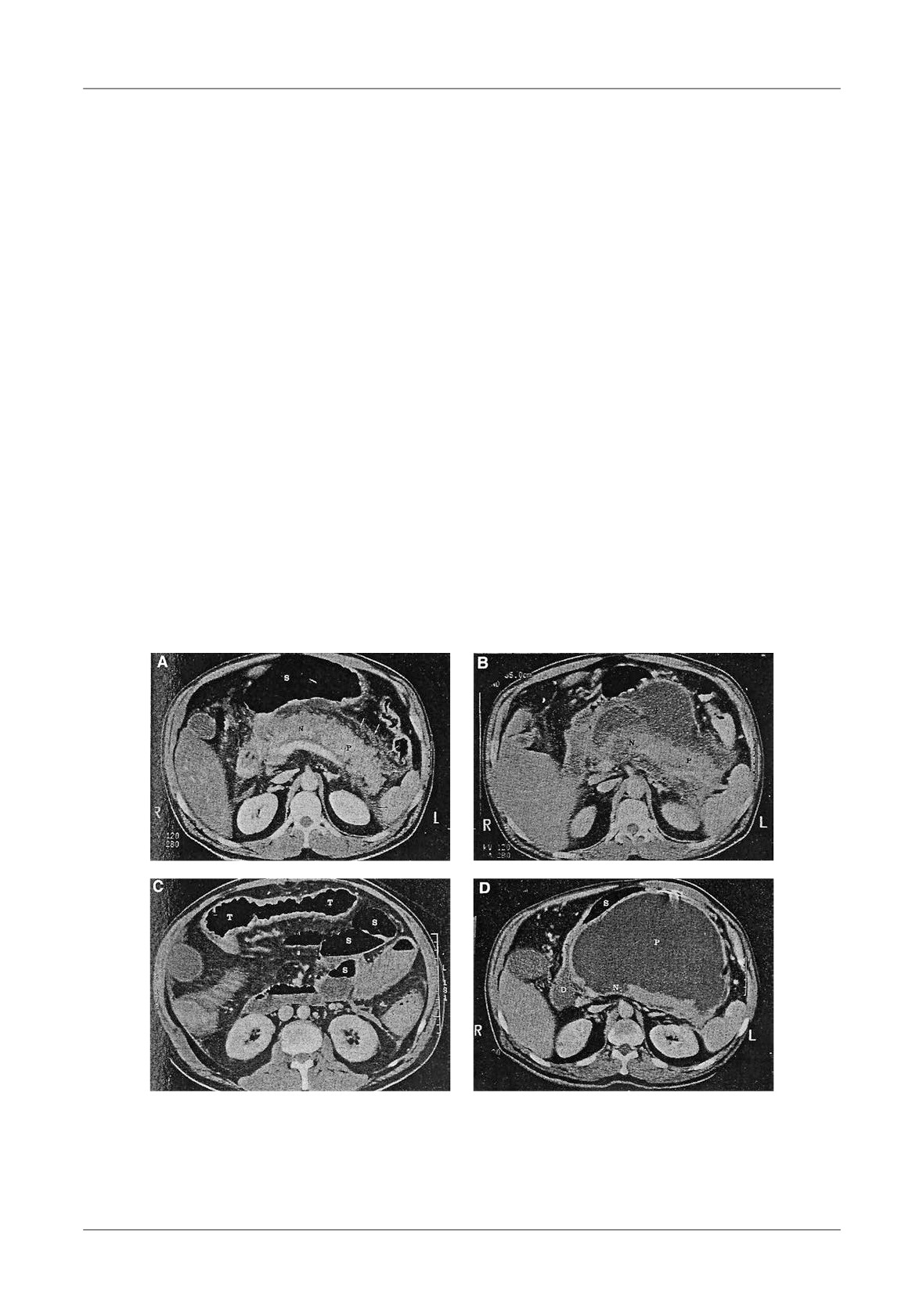
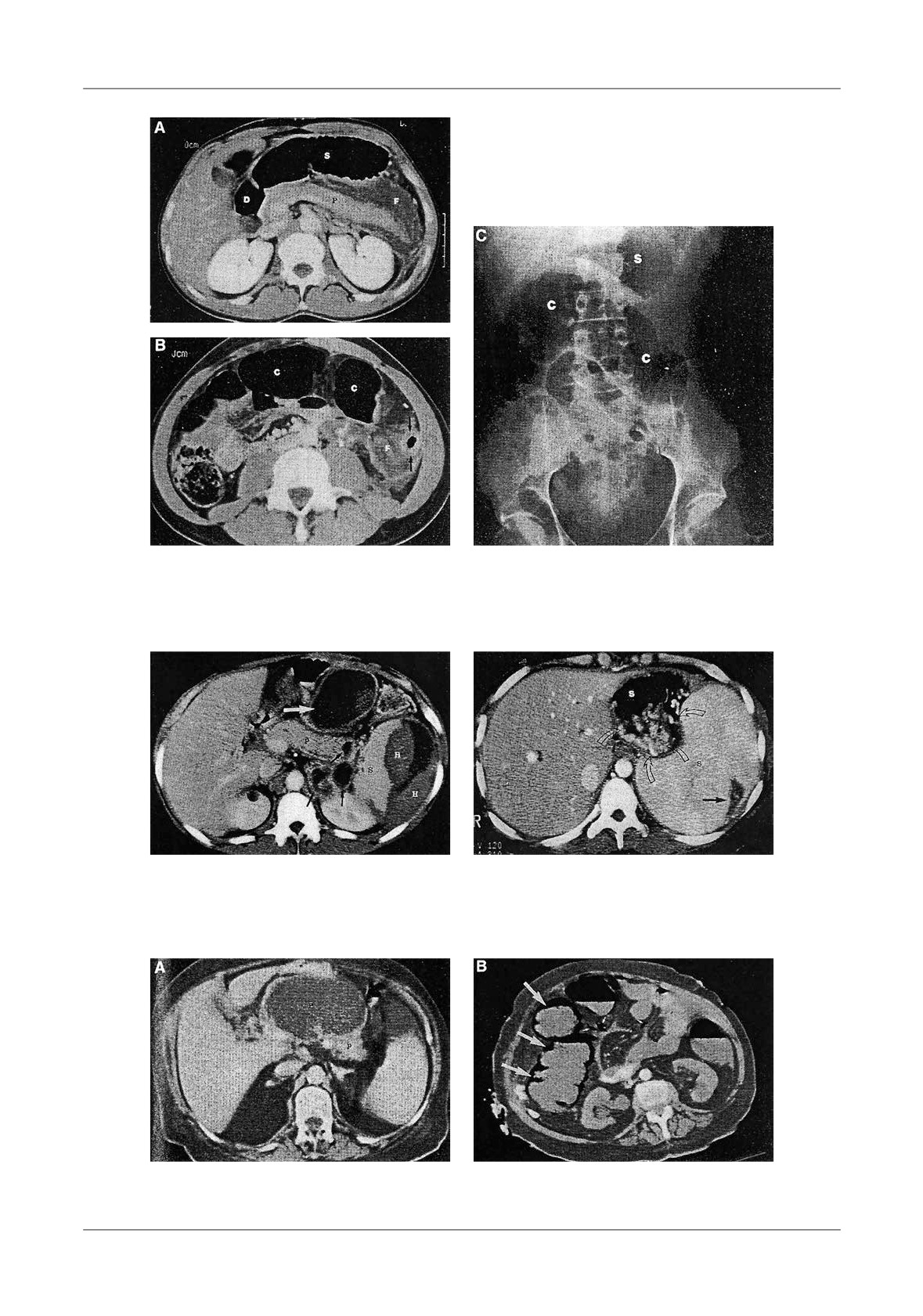
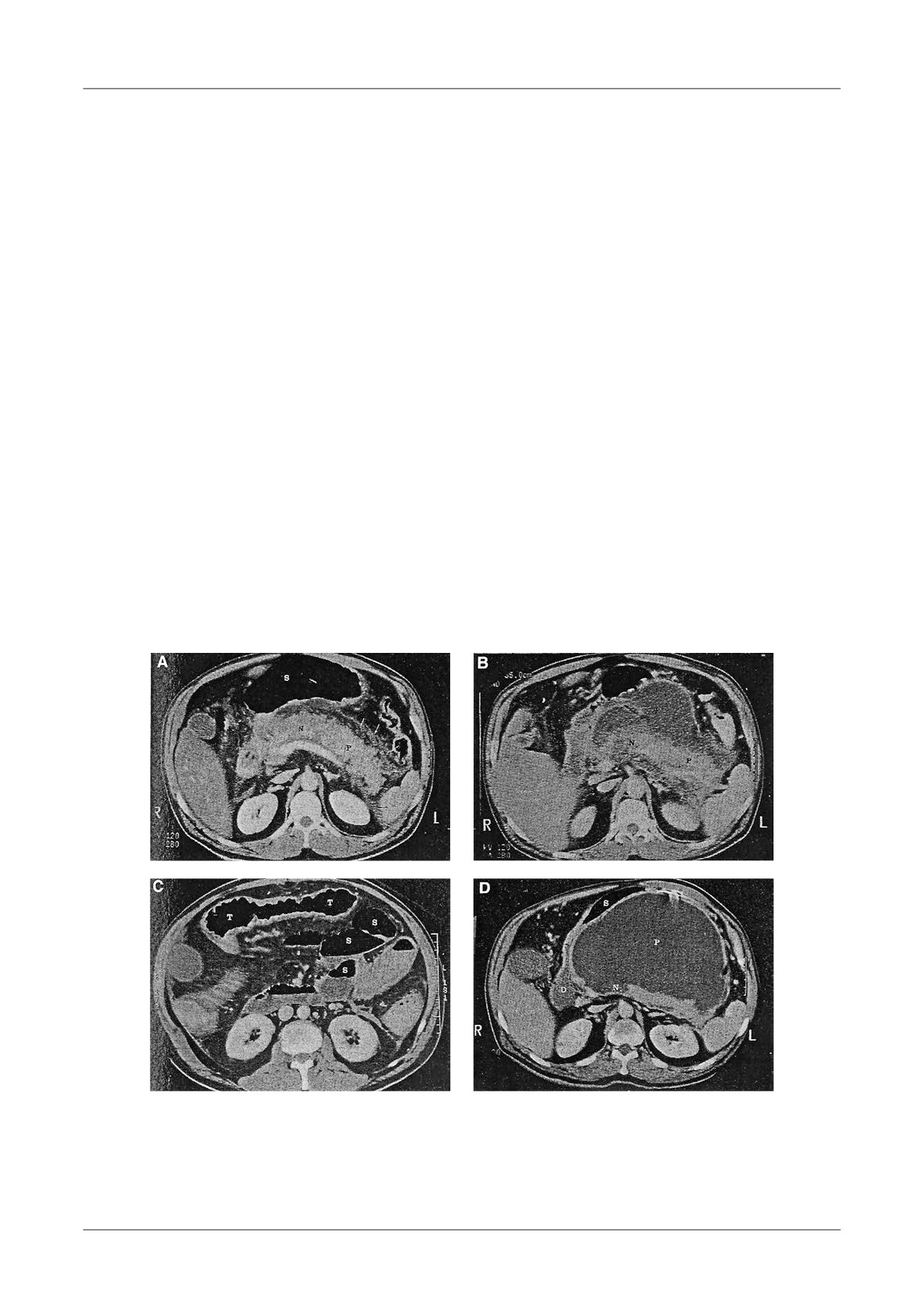
Figure 1. Pancreatic necrosis with the development of a pseudocyst, ileus and colonic in ltration in a 38
-year-old man. A-At admission the CT- shows enlarged pancreas and peripancreatic in ammation, uid
(N=necrosis, P=pancreas, S=stomach), B-Lique ed necrosis nine days later with partially encapsulated
uid collection in the lesser sac, C-Dilated small bowel loops, with a haustral transverse colon. S=small
bowel, T=transverse colon, D-Five weeks later, fully encapsulated pseudocyst in the lower sac, with
lique ed necrosis in the neck of the pancreas (D=duodenum, N=necrosis, P=pseudocyst, S=stomach)
20
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
hyperglycemia
>200 mg% (patients), hypocalcaemia
Table I. Systemic complications
<8mg % (39 cases), the levels of serum amylase and
and manifestations of acute pancreatitis
C-reactive protein
(CRP) concentrations, serum
Lesions
%
creatinine blood test values (Table I).
Pulmonary in ltrate *
40%
e mortality in the early stage: In this study, deaths
ARDS
20%
occurred in 6 patients (47%) of the average (median)
Oliguria
80%
interval of 8 days ( range 1-11) days, secondary to MSOF,
Hyperglycemia >200mg%
>50%
whereas 7 deaths (53%) occurred late at the average/
median of 55 days (range 18-80), secondary infected
Hypocalcaemia <8mg%
38%
pancreatic necrosis, and a retroperitoneal di use sepsis.
Pulmonary in ltrate*=Pulmonary in ltrate/pleural e usions
e intermediate complications occurred between the
second to the fth weeks after the attack of pancreatitis.
In this series death occurred in 1 patient with focal
Table II. e most frequent bacteria
necrosis (<30% of pancreas), 4 patients with 30% to
occurring in pancreatic infections
50% necrosis and 8 patients (52%) with >50% necrosis.
Bacteria
Number of cases (%)
In this study the secondary bacterial infection
E. Coli
14 (36.84%)
occurred in 70% of patients with necrotizing pancreatitis.
Enterobacter
10 (26.32%)
e necrosis was present in 20% of patients with 10%
Klebsiella
9 (23.68%)
secondary infected necrosis. At the evolution of the
Anaerobi
5 (13.16%)
sterile necrotic tissue, the liquefaction occurred within
Total
38 (100%)
the rst 2 to 3 days from the event. In this situation the
CT imaging depicted an area of decreased alteration
demarcating the viable tissue from the necrotic one.
We observed that, sterile necrotic tissue tended to
undergo liquefaction within the rst 2 to 3 days of
evolution, which can be depicted by CT imaging
showing the di erence between the viable from and
necrotic tissue (Figure 1).
In infected necrosis, the most commonly
incriminated bacteria are gram-negative organisms of
intestinal origin (Table II).
In patients with necrosis and secondary infection
presented with septic manifestations which developed
between the second and fourth week after the acute
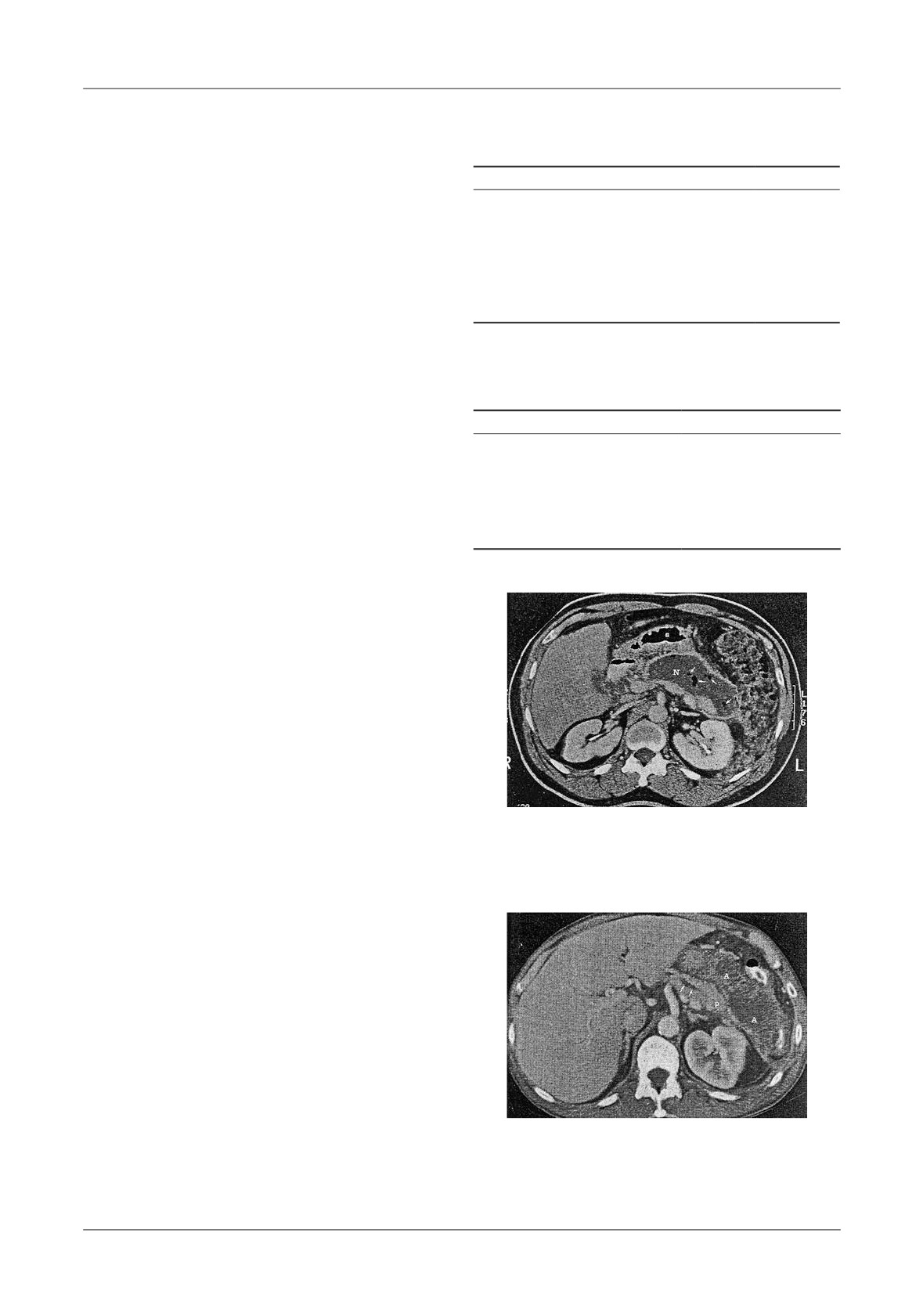
Figure 2. Infected pancreatic necrosis, more of 50% of the
onset (Fig. 2).
CT image is necrosis, with encapsulated liquefaction
According to our experience the detection of gas in
and air bubbles
the necrotic tissue was present in 12% of cases (Figure
2). Such CT ndings are indicative of infected necrosis.
e pancreatic abscess occurred in 3 patients (Figure
3), usually
3 to
4 weeks after the onset of acute
pancreatitis.
In our experience the majorities of pseudo cysts that
develop following an attack of acute pancreatitis were
associated with and evolve at the site of necrosis (Figure
1-4).
In
40% of acute pseudocysts had spontaneous
resolution and 20% were complicated, whereas pseudo
cysts present for more the
12 weeks tended not to
resolve and were associated with a complication rate of
Figure 3. Pancreatic abscess. 5 weeks following acute
65%.
pancreatitis, heterogeneous uid collection anterior to the
Cysts >6cm in diameter required surgical treatment
body and tail of the pancreas. Pancreatic ducts are distended
in more than 60%, <6cm in diameter (40%), and acute
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
21
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
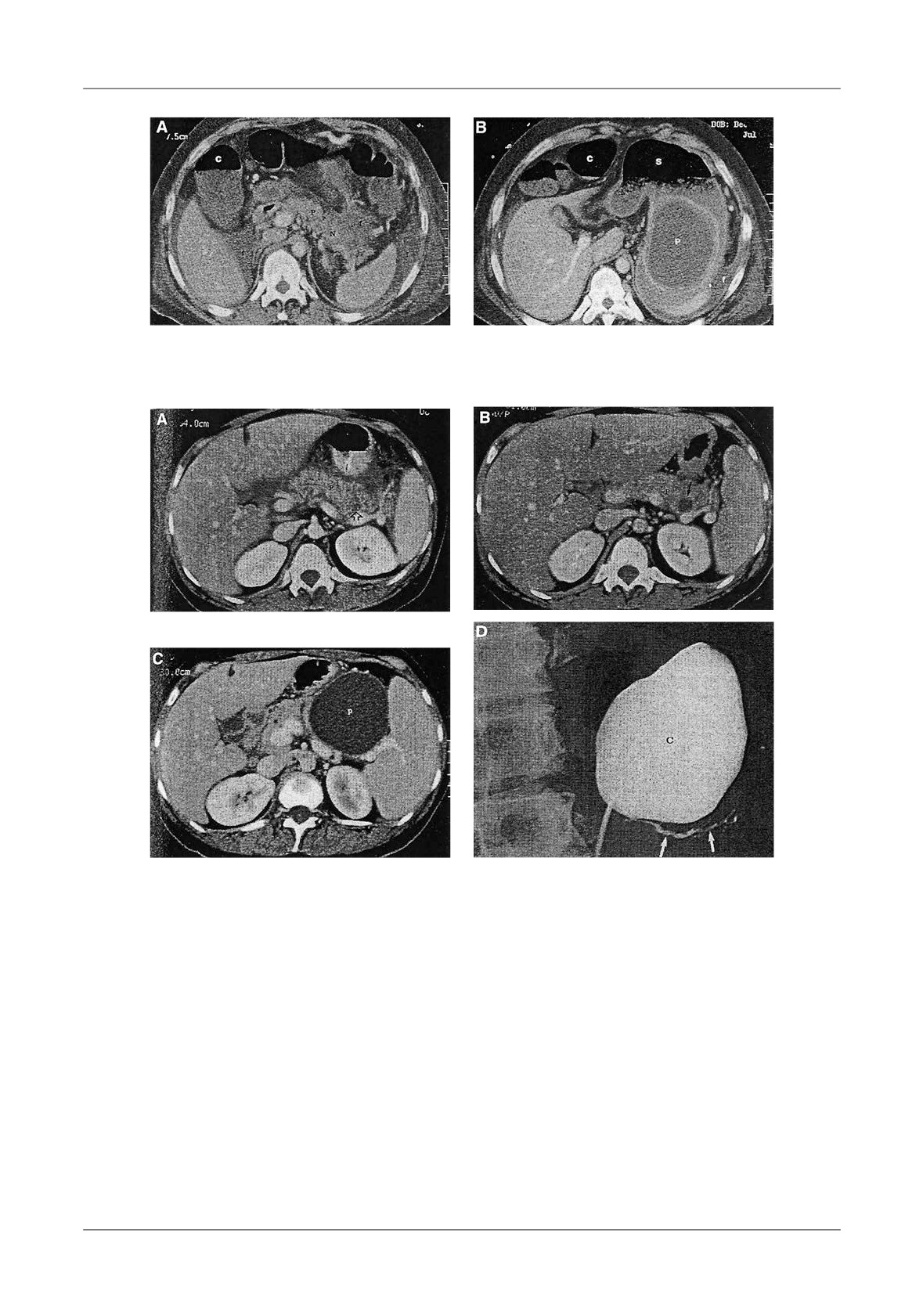
Figure 4. Pancreatic pseudocyst secondary to necrosis.
A - Liquefaction necrosis in the tail, B - Large pseudocyst bulging into the stomach
Figure 5. Pseudocyst communicating with the pancreatic duct, A-With CT image of enlarged gland
and peripancreatitis, B-After discharge from hospital, 2 weeks later, CT shows a residual collection,
C-6 months later, the patient had abdominal pain, CT shows an enlarging pseudocyst,
D-Trans gastric punction with stulography, shows communication with the Wirsung duct
pseudo cysts <5cm in size seen in asymptomatic patients
Most of the serious complications (4 cases), had the
at the end of an acute episode, were managed
tendency to occur predominantly late within a few
conservatively with CT- follow up control (Figure 5).
months to years after acute pancreatitis. In our
In 16 cases the stomach, duodenum, transverse
experience, arterial venous lumen obstruction can lead
colon involved localized spasm at the splenic exure of
to segmental colonic or proximal small bowel ischemia
the colon. is explains the signi cant distension of the
and infarction (Figure 9).
proximal air- lled transverse colon (Figure 6)
Transitory small volume ascites was relatively a
In solid organ involvement, splenic involvement
frequent CT nding, in 10 cases of the patients with AP.
was the most common because of the topography
e true pancreatic ascites can occur early, or after
between the pancreatic tail and splenic hilum (Figure 7,
several episodes of AP. In our study the patients with
8).
true ascites had increasing abdominal girth 24 cases,
22
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
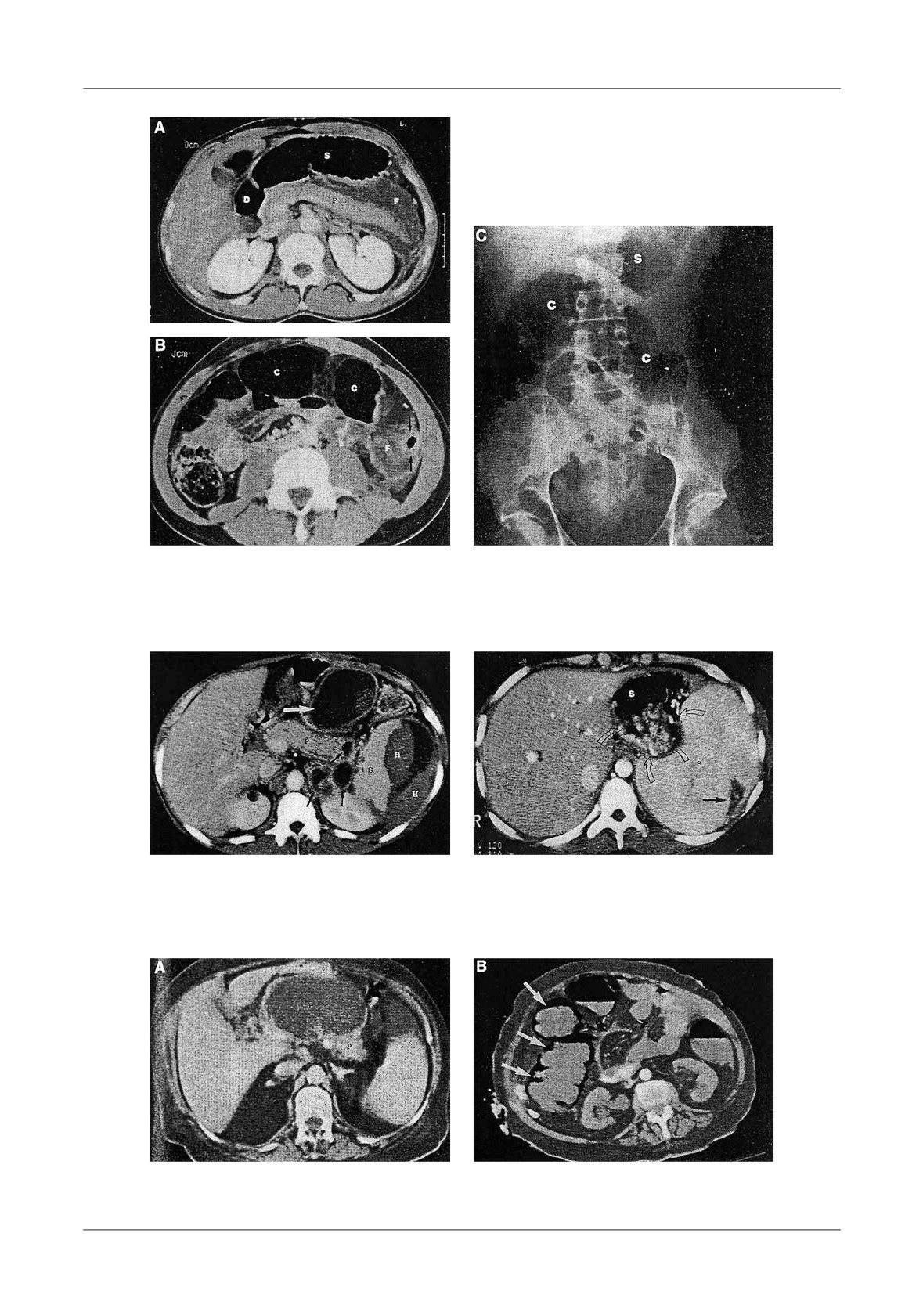
Figure 6. A - Normally enhancing pancreas with peripancreatic uid collections (D=duodenum,
S=stomach, F= uid, P=pancreas), B - Transverse colon is air lled and distended, C - Native
abdominal lm showing distension of transverse colon
Figure 7. Intrasplenic and subcapsular
Figure 8. Splenomegaly and gastric varices with
hemorrhage (H=hemorrhage, S=spleen,
two episodes of pancreatitis. Massive enlarged
P=pancreas)
spleen, with peripheral infarct
Figure 9. Infarcted right colon in A.P. A-CT image shows pseudocyst with pancreatic necrosis
6 weeks following AP, B-One month later CT showed late pneumocystosis
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
23
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
abdominal pain 24 cases, weight loss
22 cases and
in19% of patients. e diagnosis of infected pancreatic
occasional nausea or vomiting 2 cases.
necrosis was made through CT which showed air in the
retro peritoneum or retroperitoneal collections
Discussion
[34,35,36].
e presence of non enhancing areas of
solid or potentially lique ed pancreas on CT itself are
Early complications associated with multiorgan
not diagnostic of infection as demonstrated in our study
failure: (early 2-3 days, with SIRS), are responsible for
in gure 2, con rmed by the studies of Kelly et al. [37].
20-50% of the mortality [10,11,12]. e pathogenesis
In our study, the detection of gas bubbles in the
of these potentially lethal early complication is complex
necrotic tissue was observed in 12% of cases, and that
(intrapancreatic activation of digestive enzymes,
was indicative of infection, Figure 2.
systemic in ammatory response, excessive stimulating
An aggressive surgical approach is recommended to
in ammatory cells,
systemic
microcirculatory
patients with infected necrosis. Whenever possible, the
disturbances, oxidative stress, aggravating e ect of hyper
surgical intervention should be delayed until the third or
lipidemia) [13,14,15].
fourth week in the absence of clinical deterioration
e production and the release of various enzymes,
[36,38,39]. Most of the surgical strategies include
vasoactive peptides, and in ammatory mediators are
necrosectomy, debridement with segmental resection,
responsible for the development and severity of
sequestectomy, sump drainage and lavage, retro
cardiovascular, pulmonary or several dysfunctions
peritoneostomy.
ese procedures in specialized
[16,17,18].
institutions reduce the mortality rate to below 10% from
Pulmonary complications with detectable
previously reported 40% to 80% death rates [40,41,42].
pulmonary in ltrates and/or pleural e usions occur in
In 3% of cases the pancreatic abscess is present in
15% up to 55% of patients su ering from acute
the evolution of severe pancreatitis, usually 3 to 4 weeks
pancreatitis
[19,20,21]. Profound respiratory failure
after the onset of AP when peripancreatic uid
with ARDS- syndrome occurs in up to 20% in acute
collections are present
[43,44]. A pancreatic abscess
pancreatitis [21].
should be suspected using CT when uid collections of
Renal complications, with oliguria, can progress to
di erent sizes are depicted in septic patients with a
acute renal failure, which carries a mortality of 80%
recent (3-4 weeks) history of pancreatitis as demonstrated
[22,23].
in our study, and con rmed also in Banks’ study [45].
Severe intra abdominal or gastrointestinal
Failure of resorbtion of extravasated pancreatic
hemorrhage is an abnormal early complication, and
secretions and the presence of a communicating tract
other hemorrhagic complications occur in
25% of
with the pancreatic ductal system can explain the
patients with poor prognosis [24,25].
development of pseudocysts
(Figure
4,5). In our
In acute pancreatitis, the hypocalcaemia de ned as
experience the majorities of pseudo cysts were associated
serum calcium <8mg/dL, occur early, and represents a
with parenchymal necrosis and evolve at those sites,
reliable prognostic indicator of disease severity [26,27]
Figures 1,4,5.
and high mortality rates are expected in patients with
Surgical or percutaneous drainage is reserved for
calcium levels <7mg/dL.
cysts larger than
5cm older than
6 weeks and
Detection of the mentioned early systemic
symptomatic, pain, abdominal mass, gastric outlet
complications (Table II) has led to speci c treatment
obstruction, infection or hemorrhage [46]. e presence
options.
of hemorrhagic pseudocyst was 18% in our series of 103
e most frequent indication for intervention in
cysts. In other reports pseudocysts developed in 2% to
severe acute pancreatitis is infected pancreatic necrosis,
31% [37,43,47,48].
and this is a risk factor for abdominal compartment
Proteolytic action of the extravasated pancreatic
syndrome due to visceral and retroperitoneal edema
secretions can explain the gastrointestinal and biliary
[26,27,28] Failure of no operative management mandates
complications in acute pancreatitis, and most of the
abdominal decompression. is complication is associated
abnormality involving the stomach, duodenum, and
with a very high rate of MSOF and death [29,30,31].
transverse colon, Figure 1, suggested by Aly et al. study
Pancreatic necrosis occurs later in the evolution,
in 2002 [49].
most commonly in the third to fourth week of the
Vascular complications in evolution of acute
disease [32,33].
pancreatitis are infrequent; they can result in high
In our study, patients with infected necrosis, the
mortality rates if not detected early, with evolution to
infection was detected within the rst 2 weeks of illness
pseudo aneurysm and massive hemorrhage [50,51].
24
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Most of the major hemorrhagic complications are
11.
Liu TH, Kwong KL, Tamm EP, Gill BS, Brown SD,
secondary to a bleeding pseudo aneurysm, with a
Mercer DW. Acute pancreatitis in intensive care unit
reported incidence as high as 10% [52]. Intraabdominal
patients: value of clinical and radiologic prognosticators
hemorrhage can be identi ed early by CT imaging [41].
at predicting clinical course and outcome. Crit Care
e incidence of transitory ascites is a relatively
Med 2003;31(4):1026-30.
frequent CT nding but true pancreatic ascites rarely
12.
Buter A, Imrie CW, Carter CR, Evans S, McKay CJ.
occurs [53].
Dynamic nature of early organ dysfunction determines
outcome in acute pancreatitis. Br J Surg 2002;89(3):298-
Conclusions
302.
13.
Johnson CD, Abu-Hilal M. Persistent organ failure
Mortality in acute pancreatitis dependents on
during the rst week as a marker of fatal outcome in
potentially lethal complications and that can coexist and
acute pancreatitis. Gut 2004;53(9):1340-4.
occur any time in evolution of pancreatitis. ey can be
14.
Brown A, Orav J, Banks PA. Hemoconcentration is an
divided into: early complications that manifest
early marker for organ failure and necrotizing
themselves within the rst
2-3 days; intermediate
pancreatitis. Pancreas 2000;20(4):367-72.
complications during the second to fth week; late
15.
Papachristou GI, Whitcomb DC. In ammatory
complications, that occur within months or years after
markers of disease severity in acute pancreatitis. Clin
the resolution of an acute episode.
Lab Med 2005;25(1):17-37.
e early detection by clinical imaging methods
16.
Mayer J, Rau B, Gansauge F, Beger HG. In ammatory
leads to speci c treatment options.
mediators in human acute pancreatitis: clinical and
pathophysiological implications. Gut 2000;47(4):546-
52.
References
17.
Malfertheiner P, Domínguez-Muñoz JE. Prognostic
factors in acute pancreatitis. Int J Pancreatol 1993;14(1):1-8.
1.
Halonen KI, Pettilä V, Leppäniemi AK, Kemppainen
18.
Banks PA, Martin L, Freeman L, et al. Practice
EA, Puolakkainen PA, Haapiainen RK. Multiple
Guidelines in Acute Pancreatitis. Am J Gastroenterol
organ dysfunction associated with severe acute
2006;101(10):2379-400.
pancreatitis. Crit Care Med 2002;30(6):1274-9.
19.
Talamini G, Bassi C, Falconi M, et al. Risk of death
2.
Balthazar EJ, Robinson DL, Megibow AJ, Ranson
from acute pancreatitis. Int J Pancreatol 1996;19(1):15-
JH. Acute pancreatitis: value of CT in establishing
24.
prognosis. Radiology 1990;174(2):331-6.
20.
Vriens PW, van de Linde P, Slotema ET, Warmerdam
3.
Buggy BP, Nostrant TT. Lethal pancreatitis. Am J
PE, Breslau PJ. Computed tomography severity index is
Gastroenterol 1983;78(12):810-4.
an early prognostic tool for acute pancreatitis. J Am Coll
4.
McKay CJ, Evans S, Sinclair M, Carter CR, Imrie
Surg 2005;201(4):497-502.
CW. High early mortality rate from acute pancreatitis in
21.
Pastor CM, Matthay MA, Frossard JL. Pancreatitis-
Scotland, 1984-1995. Br J Surg 1999;86(10):1302-5.
associated acute lung injury: new insights. Chest
5.
Denham W, Norman J. e potential role of therapeutic
2003;124(6):2341-51.
cytokine manipulation in acute pancreatitis. Surg Clin
22.
Buter A, Imrie CW, Carter CR, Evans S, McKay CJ.
North Am 1999;79(4):767-81.
Dynamic nature of early organ dysfunction determines
6.
Connor S, Alexakis N, Raraty MG, et al. Early and
outcome in acute pancreatitis. Br J Surg 2002;89(3):298-
late complications after pancreatic necrosectomy. Surgery
302.
2005;137(5):499-505.
23.
Lin HY, Lai JI, Lai YC, Lin PC, Tang GJ. Acute renal
7.
Beger HG, Rau B, Mayer J, Pralle U. Natural course of
failure in severe pancreatitis: A population-based study.
acute pancreatitis. World J Surg 1997;21(2):130-5.
Ups J Med Sci 2011;116(2):155-9.
8.
Lowham A, Lavelle J, Leese T. Mortality from acute
24.
Gadacz TR, Trunkey D, Kie er RF Jr. Visceral vessel
pancreatitis. Int J Pancreatol 1999;25(2):103-6.
erosion associated with pancreatitis. Case reports and a
9.
Rocha FG, Benoit E, Zinner MJ, et al. Impact of radiologic
review of the literature. Arch Surg 1978;113:1438-40.
intervention on mortality in necrotizing pancreatitis: the
25.
Whitcomb DC. Acute Pancreatitis. N Engl J Med
role of organ failure. Arch Surg 2009;144(3):261-5.
2006 18;354(20):2142-50.
10.
Matull WR, Pereira SP, O’Donohue JW. Biochemical
26.
McMahon MJ, Woodhead JS, Hayward RD. e
markers of acute pancreatitis. J Clin Pathol
nature of hypocalcaemia in acute pancreatitis. Br J Surg
2006;59(4):340-4.
1978;65(3):216-8.
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
25
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
27.
Nathens AB, Curtis JR, Beale RJ, et al. Management
Symposium on Acute Pancreatitis, Atlanta, Ga,
of the critically ill patient with severe acute pancreatitis.
September
11 through
13,
1992. Arch Surg
Crit Care Med 2004;32(12):2524-36.
1993;128(5):586-90.
28.
Büchler MW, Gloor B, Müller CA, Friess H, Seiler
41.
Singla A, Csikesz NG, Simons JP, et al. National
CA, Uhl W. Acute necrotizing pancreatitis: treatment
hospital volume in acute pancreatitis: analysis of the
strategy according to the status of infection. Ann Surg.
Nationwide Inpatient Sample
1998-2006. HPB
2000; 232(5):619-26.
(Oxford) 2009;11(5):391-7.
29.
Ashley SW, Perez A, Pierce EA, et al. Necroziting
42.
Papachristou GI, Takahashi N, Chahal P, Sarr MG,
pancreatitis. Ann Surg 2001;234(4):572-80.
Baron TH. Peroral endoscopic drainage/debridement of
30.
Hungness ES, Robb BW, Seeskin C, Hasselgren PO,
walled-o
pancreatic
necrosis.
Ann Surg
Luchette FA. Early debridement for necrotizing
2007;245(6):943-51.
pancreatitis: is it worthwhile? J Am Coll Surg
43.
Crass RA, Way LW. Acute and chronic pancreatic
2002;194(6):740-4.
pseudocysts are di erent. Am J Surg 1981;142(6):660-
31.
Bakker OJ, van Santvoort HC, Besselink MG, van
3.
der Harst E, Hofker HS, Gooszen HG; Dutch
44.
Bucher P, Pugin F, Morel P. Minimally invasive
Pancreatitis Study Group. Prevention, detection, and
necrosectomy for infected necrotizing pancreatitis.
management of infected necrosis in severe acute
Pancreas 2008;36(2):113-9.
pancreatitis. Curr Gastroenterol Rep 2009;11(2):104-
45.
Banks PA. Acute pancreatitis: medical and surgical
10.
management. Am J Gastroenterol
1994;89(8
32.
Werner J, Feuerbach S, Uhl W, Büchler MW.
Suppl):S78-85.
Management of acute pancreatitis: from surgery to
46.
Whitcomb DC. Clinical practice. Acute pancreatitis. N
interventional intensive care. Gut 2005;54(3):426-36.
Engl J Med 2006;354(20):2142-50.
33.
De Waele JJ, Hoste E, Blot SI, Decruyenaere J,
47.
Kiviluoto T, Kivisaari L, Kivilaakso E, Lempinen M.
Colardyn F. Intra-abdominal hypertension in patients
Pseudocysts in chronic pancreatitis. Surgical results in
with severe acute pancreatitis. Critical Care
102 consecutive patients. Arch Surg 1989;124(2):240-
2005;9(4):452-7.
3.
34.
Besselink MG, Verwer TJ, Schoenmaeckers EJ et al.
48.
Triester SL, Kowdley KV. Prognostic factors in acute
Timing of surgical intervention in necrotizing
pancreatitis. J Clin Gastroenterol 2002;34(2):167-76.
pancreatitis. Arch Surg 2007;142(12):1194-201.
49.
Aly EA, Milne R, Johnson CD. Non-compliance with
35.
Hartwig W, Maksan SM, Foitzik T, Schmidt J,
national guidelines in the management of acute
Herfarth C, Klar E. Reduction in mortality with
pancreatitis in the United kingdom. Dig Surg
delayed surgical therapy of severe pancreatitis. J
2002;19(3):192-8.
Gastrointest Surg 2002;6(3):481-7.
50.
Cornu-Labat G, Kasirajan K, Simon R, Smith DJ,
36.
Besselink MG, van Santvoort HC, Witteman BJ,
Herman ML, Rubin JR. Acute mesenteric vein
Gooszen HG; Dutch Acute Pancreatitis Study Group.
thrombosis and pancreatitis. A rare association. Int J
Management of severe acute pancreatitis: it’s all about
Pancreatol 1997;21(3):249-51.
timing. Curr Opin Crit Care 2007;13(2):200-6.
51.
Burke JW, Erickson SJ, Kellum CD, Tegtmeyer CJ,
37.
Kelly SB, Gauhar T, Pollard R. Massive intraperitoneal
Williamson BR, Hansen MF. Pseudoaneurysms
hemorrhage from a pancreatic pseudocyst. Am J
complicating pancreatitis: detection by CT. Radiology
Gastroenterol 1999;94(12):3638-41.
1986;161(2):447-50.
38.
Bassi C. Infected pancreatic necrosis. Int J Pancreatol
52.
White AF, Baum S, Buranasiri S. Aneurysms secondary
1994;16(1):1-10.
to
pancreatitis.
AJR Am J Roentgenol
39.
Uhl W, Warshaw A, Imrie C, et al. IAP Guidelines for
1976;127(3):393-6.
the Surgical Management of Acute Pancreatitis.
53.
Johst P, Tsiotos GG, Sarr MG. Pancreatic ascites: a rare
Pancreatology 2002;2(6):565-73.
complication of necrotizing pancreatitis. A case report
40.
Bradley EL 3rd. A clinically based classi cation system
and review of the literature. Int J Pancreatol
for acute pancreatitis. Summary of the International
1997;22(2):151-4.
26
Sârbu et al
ORIGINAL ARTICLES
TREATMENT OF NOCTURIA IN A MALE GROUP OF PATIENTS WITH
LOWER URINARY TRACT SYMPTOMS LUTS . SHORT TERM RESULTS
Vasile Dan Stanca, Andrei Boc, Radu Aurel Maxim, Vitalie Gherman, Sergiu Nicolescu, Ioan Coman
Urology Department, Clinical Municipal Hospital Cluj-Napoca, Romania
Address for correspondence:
Vasile Dan Stanca
Urology Department, Clinical Municipal Hospital Cluj-Napoca
11 Tăbăcarilor Street, 400139, Cluj-Napoca
Phone: +40.744.622.933, Fax +40.264.485.295
Email: vasilestanca@yahoo.com
Received: 01.02.2014
Accepted: 20.02.2014
Med Con March 2014 Vol 9, No 1, 27-30
Abstract
irritative nocturia associated with frequency and urgency.
All patients with nocturnal polyuria reported a reduction
Nocturia is a major problem in men su ering of
in the number of times they had to wake up to urinate; 4
low urinary symptoms (LUTS). At least a third of these
patients of 6 with nocturnal irritative polakiuria also had
patients have nocturia. e etiology of this condition is
positive response to the therapy. We did not record any
under debate with several mechanisms of occurrence
cardio-vascular or urological side e ects.
being taken into account. We have evaluated the results
Conclusions: Our results suggest that treatment
of treatment in patients that complained mainly of this
with desmopressin 60/120 micrograms/day is e ective
symptom.
in patients with secondary nocturnal urinations due to
Material and Methods: We have evaluated a
nocturnal polyuria.
e treatment with desmopresin
number of 29 male patients aged 50 years or older. ey
was well tolerated. Identifying the pathophysiological
complained of having to wake up at night to urinate
mechanism of nocturia is essential for establishing an
(sole symptom or associated with other LUTS).
e cient treatment.
Standard diagnostic workout included bladder voiding
Keywords: nocturia, lower urinary tract symptoms,
diary.
e rst groups of patients with nocturia due to
desmopressin, alpha blockers, antimuscarinics
nocturnal polyuria or with a nocturnal diuresis superior
to 400 mL were treated with desmopressin 60 or 120
Introduction
micrograms/day for
30 days.
e second group of
patients with small volume nocturnal nicturition was
Nocturia, de ned by the International Continence
treated with alpha blockers with antimuscarinics. We
Society as “the complaint that the individual has to
evaluated the results and the side e ects of this
wake at night one or more times to void”, is a common
treatment.
and bothersome symptom with a signi cant impact on
Results: Of the total number of patients with
sleep-quality and quality of life [1]. It is a prevalent
bothersome nocturnal urination episodes
79.3% (23
condition; however, it often goes unreported [2].
patients) presented secondary nocturia due to nocturnal
Traditionally it was considered as a benign prostatic
polyuria
(1-5 urinations per night);
6 patients had
hyperplasia (BPH) - related condition and the treatment
Treatment of Nocturia in a Male Group of Patients With Lower Urinary Tract Symptoms (LUTS). Short-Term Results
27
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
was prostate-centered accordingly. e item no. 7 in the
medical treatment in patients complaining of nocturia
International Prostatic Symptom Score
(IPSS
(sole symptom or associated with other LUTS), the
questionnaire) speci cally addresses the issue of
treatment decision being driven by the mechanism of
nocturnal voiding (“During the last month how many
occurrence of the nocturnal micturitions.
times did you most typically get up to urinate from the time
you went to bed at night until the time you got up in the
Material and Methods
morning?”). In the last decade however the path
physiology of nocturia was better understood and
We included in the study men aged 50 years or
several other factors beside the prostate were
older complaining with nocturnal complains sole
incriminated for causing it.
e nocturnal polyuria,
symptom or associated with other LUTS. We excluded
overactive bladder syndrome or non-urological
from the study the patients with conditions that would
conditions such as arterial hypertension or congestive
require a speci c treatment: urinary tract infections,
heart failure were in turn studied as etiologic factors [3].
known or suspected urological malignancies, signi cant
is broader, more complex approach to the
bladder outlet obstruction with post-void residual urine
pathogenesis of nocturia was triggered by several
>100 mL and reduced functional bladder capacity and
observations. First, it is almost as prevalent in women as
the patients with co morbidities that could interfere
it is in men. In a Finnish study the age standardized
with the use of antimuscarinics, alpha 1 blockers or
prevalence of nocturia (1 or more voids per night) was
desmopressin (glaucoma, hyponatremia).
approximately 40% for both genders. It was even more
Standard diagnostic workout included medical
common in young women than in men; in the 50-59
history,
physical examination, ultrasonographic
years age group the incidence was equal, half of men
measurement of the post-void residual urine and the
and women reported nocturia, whereas after 60 years of
bladder voiding diary.
e latter was a pivotal test,
age the men were signi cantly more a ected [4]. is
allowing us to de ne two groups of patients: patients
pattern of evolution suggests both the presence of other,
with nocturia due to nocturnal polyuria or with a
non-prostatic etiologic factors and the implication of
nocturnal diuresis superior to 400 mL, and a second
the prostatic pathology in the aging male.
group with small volume nocturnal micturitions.
e overactive bladder syndrome is another
Patients of the rst group were treated with
condition that can lead to nocturnal micturitions. e
desmopressin 60 micrograms/day (if their age was >65
International Continence Society
(ICS) de nes
years) or 120 micrograms/day (ages below 65 years) for
overactive bladder syndrome (OAB) as an association of
30 days; patients with small volume nocturnal
symptoms including “urgency, with or without urge
micturitions were treated with a combination of alpha 1
incontinence, usually with increased frequency and
blockers and antimuscarinics. We monitored the sodium
nocturia” [5]. e typical nding in these cases is small
serum level for all patients with desmopressin after 7
volume nocturnal micturitions.
e condition is very
days of treatment.
often encountered in OAB patients, approximately 75%
e endpoint of the study was the reduction of the
of them reporting one or more nocturia episodes per
number of nocturnal micturitions by at least one
night [6].
episode/night. In this respect we tried to treat the
Several non-urologic conditions have been recently
patients according to the suspected pathophysiological
incriminated in the etiology of nocturnal micturitions.
mechanism rather than etiology.
Epidemiologic studies reported a signi cant relationship
We evaluated the results and the side e ects of this
between nocturia and such conditions as arterial
treatment; the patients were re-evaluated using the same
hypertension or sleep-disordered breathing. e cause-
protocol after 30 days.
and-e ect relationship between them has not been yet
established, but the e ects of arterial hypertension on
Results
glomerular ltration and tubular transport, atrial stretch
and release of atrial natriuretic peptide and peripheral
We evaluated 29 male patients aged 53-84 years
edema may all play a role in the occurrence of nocturnal
that presented with nocturia in our service between
micturitions [7,8].
January 2011 and April 2012.
Since the condition is highly multifactorial, the
23 patients
(79.3%) with bothersome nocturnal
treatment decision should take into account all the
urination episodes had secondary nocturia due to
possible etiological factors. Bearing in mind all of this
increased nocturnal diuresis (over 400 mL urine/night).
considerations, we decided to evaluate the results of
e nocturnal diuresis for this group of patients ranged
28
Stanca et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
from 400 to 1200 mL. Ten of these were >65 years of
(desmopressin) o ers the chance of a signi cant
age and received 60 micrograms of desmopressin/day;
symptomatic relief [13]. e molecule was investigated
the 13 remaining patients received a daily dose of 120
for this role in the last 10 years and the safety pro le was
micrograms/day. All of these patients reported a
established [14].
e main limitation in its use is the
reduction by at least one episode in their nocturia after
risk of hyponatremia that could be higher in patients
30 days of treatment with desmopressin.
over
65 years. Several recent reports alleviate the
Six patients (20.7%) had low-volumes nocturnal
concerns: the women have higher risk than men and a
micturitions associated with frequency and urgency.
low dose of
60 micrograms/day could be safely
Four out of these 6 patients was respondent positively to
prescribed to men of any age without increased risk of
the therapy, a reduction by at least one nicturition
electrolyte imbalance [15]. In our study we used the low
episode per night. e remaining two patients declared
dose of 60 micrograms of desmopressin/day for men
that their symptoms were unin uenced by the therapy.
over 65 years and did not record hyponatremia or any
We did not record any cardio-vascular or urological
other side e ects.
side e ects.
e serum level of sodium was
>130
When the storage capacity of the bladder seems
mmol/L for all patients after 7 days of treatment.
impaired the combination therapy with alpha blockers
and antimuscarinics o ers the best results [16].
e
Discussion
majority of our patients within this group had
symptomatic improvement after 30 days of treatment.
e treatment of nocturia has always been a
challenge for the urologist. e early treatment concepts
Conclusions
included the nocturnal micturitions amid the symptoms
caused by the bladder outlet obstruction, so that a
e majority of the patients had nocturia due to
reduction of the number of nocturnal micturitions was
high nocturnal urine output. Our results suggest that
expected from treatments aimed in cases of BPH. e
treatment with desmopresin 60/120 micrograms/day is
alpha blockers yielded disappointing results: the net
e ective in patients with secondary nocturnal urinations
reduction in the number of nocturnal micturitions was
due to increased nocturnal urine output. e treatment
0.3/night over placebo for terazosin or terazosin with
with desmopresin was well tolerated. e alpha blockers
nasteride in a study published as early as 2003 [9] and
and antimuscarinics should be administered only to the
the results were duplicated by others [10].
patients complaining of frequency and urgency.
When the urinary bladder was responsible for the
Identifying the pathophysiological mechanism of
condition, the antimuscarinics were prescribed to all
nocturia is essential for establishing an e cient
patients with nocturia.
e results were equally
treatment. It is our opinion that in case of men with
disappointing, the net bene t over placebo being a
nocturia the treatment decision should be guided by the
reduction in the number of nocturnal micturitions by
underlying pathophysiological mechanism, rather than
0.05-0.29 times for di erent molecules
(solifenacin,
strict anatomical or etiological considerations.
trospium chloride etc) [11,12].
is condition is multifactorial and many of the
Conflict of Interest
etiologic factors are for the time being either unknown
or beyond therapy. Such as was impaired release of atrial
e authors have nothing to disclose.
natriuretic peptide. We believe that the only possible
way to approach nocturia is to try to identify the
mechanism of occurrence: increased nocturnal diuresis
References
(over the functional bladder capacity), overactive
bladder (low-volume micturitions) or residual urine that
1. van Kerrebroeck P, Abrams P, Chaikin D, et al. e
reduces arti cially the bladder storage capacity.
e
standardization of terminology in nocturia: report from
latter situation can be easily identi ed by abdominal
the Standardization Sub-committee of the International
ultrasound and has speci c treatment; for the former
Continence
Society.
Neurourol
Urodyn
two situations the frequency-volume charts are
2002;21(2):179-83.
invaluable tools for treatment selection.
2. van Doorn B, Bosch JL. Nocturia in older men.
For the patients with nocturia and high nocturnal
Maturitas 2012;71(1):8-12.
urine output (we believe that 400 mL urine/night would
3. Cornu JN, Abrams P, Chapple CR et al. A
be a practical threshold) only the antidiuretic therapy
contemporary assessment of nocturia: de nition,
Treatment of Nocturia in a Male Group of Patients With Lower Urinary Tract Symptoms (LUTS). Short-Term Results
29
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
epidemiology, pathophysiology, and management--a
10.
Park HK, Kim HG. Current evaluation and treatment
systematic review and meta-analysis. Eur Urol
of nocturia. Korean J Urol 2013;54(8):492-8.
2012;62(5):877-90.
11.
Brubaker L, FitzGerald MP. Nocturnal polyuria and
4.
Tikkinen KA, Tammela TL, Huhtala H, Auvinen A.
nocturia relief in patients treated with solifenacin for
Is nocturia equally common among men and women? A
overactive bladder symptoms. Int Urogynecol J Pelvic
population based study in Finland. J Urol
Floor Dysfunct 2007;18(7):737-41.
2006;175(2):596-600.
12.
Rudy D, Cline K, Harris R, Goldberg K, Dmochowski
5.
Natalin R, Lorenzetti F, Dambros M. Management of
R. Multicenter phase III trial studying trospium chloride
OAB in ose Over Age
65. Curr Urol Rep
in patients with overactive bladder. Urology
2013;14(5):379-85.
2006;67(2):275-80.
6.
Irwin DE, Abrams P, Milsom I, Kopp Z, Reilly K.
13.
van Kerrebroeck P, Rezapour M, Cortesse A, üro
EPIC Study Group. Understanding the elements of
J, Riis A, Nørgaard JP. Desmopressin in the treatment of
overactive bladder: questions raised by the EPIC study.
nocturia: a double-blind, placebo-controlled study. Eur
BJU Int 2008;101(11):1381-7.
Urol 2007;52(1):221-9.
7.
Feldstein CA. Nocturia in arterial hypertension: a
14.
Mattiasson A, Abrams P, Van Kerrebroeck P, Walter S,
prevalent, underreported, and sometimes underestimated
Weiss J. E cacy of desmopressin in the treatment of
association. J Am Soc Hypertens 2013;7(1):75-84.
nocturia: a double-blind placebo-controlled study in
8.
Parthasarathy S, Fitzgerald M, Goodwin JL, Unruh
men. BJU Int 2002;89(9):855-62.
M, Guerra S, Quan SF. Nocturia, sleep-disordered
15.
Juul KV, Klein BM, Sandström R, Erichsen L,
breathing, and cardiovascular morbidity in a
Nørgaard JP. Gender di erence in antidiuretic response
community-based cohort. PLoS One 2012;7(2):e30969.
to desmopressin. Am J Physiol Renal Physiol
9.
Johnson TM 2nd, Jones K, Williford WO, Kutner
2011;300(5):F1116-22.
MH, Issa MM, Lepor H. Changes in nocturia from
16.
Van Kerrebroeck P, Haab F, Angulo JC, et al. E cacy
medical treatment of benign prostatic hyperplasia:
and safety of solifenacin plus tamsulosin OCAS in
secondary analysis of the Department of Veterans
men with voiding and storage lower urinary tract
A airs Cooperative
Study Trial.
J
Urol
symptoms: results from a phase 2, dose- nding study
2003;170(1):145-8.
(SATURN). Eur Urol 2013;64(3):398-407.
30
Stanca et al
ORIGINAL ARTICLES
FINITE ELEMENT ANALYSIS OF A NEW EXPANDABLE INTERBODY
FUSION CAGE
Mihai Magureanu1, Dinu Vermesan2, Juganaru Iulius2, Horia Haragus2, Roberta Cecilia Avram4,
Dan Ioan Stoia3, Gigi Adrian Aiordachioaie4
1University of Medicine and Pharmacy “Carol Davila” Bucharest, 2University of Medicine and Pharmacy “Victor Babeş”
Timişoara, 3Politechnic University Timişoara, 4West University “Vasile Goldiş” Arad
Address for correspondence:
Haragus Horia
Ist Clinic of Orthopedics and Trauma,
Emergency Clinical County Hospital Timişoara
10 Iosif Bulbuca Blvd, 300736, Timişoara, România
Phone: +40747025064, fax +40256487144
E-mail: horia.haragus@yahoo.com
Received: 01.11.2013
Accepted: 15.01.2014
Med Con March 2014 Vol 9, No 1, 31-35
Abstract
Keywords: lumbar fusion, posterior lumbar
interbody fusion
(PLIF), transforaminal lumbar
Chronic low back pain is caused by degeneration of
interbody fusion (TLIF)
the lumbar segments. e current trends are focusing on
minimal invasive surgery.
erefore, we aimed to
Introduction
determine the impact on the adjacent disc of a newly
designed expandable TLIF
(transforaminal lumbar
Chronic low back pain is caused by degeneration of
interbody fusion) cage using nite element modeling.
the lumbar segments. Many known factors contribute
e numerical simulations were performed comparative
while for some instances the etiopathogenesis is unclear.
for two di erent structures: cage closed and expanded to
Disc degeneration is the main cause, followed by
degrees.
is led to the L4-L5 endplates being parallel
apophyseal arthritis. As the disc degenerates it can
and with a 4.2 lordosis respectively. All other parameters
herniate and thus cause focal compression. When this
were kept constant. For each situation we performed 12
progresses the disc collapses and the foramens and the
simulations aimed at reproducing di erent grades of
spinal canal become narrower. e zygomatic joints can
lumbar spine exion. We de ned rotation angles for the
easily be the source of pain themselves. As they
L3 vertebra and kept the fused L4-L5 segment rigid.
degenerate the foramens can be narrowed and the
e e ects were measured in the elastic deformation
proximal segment can slide anteriorly leading to spinal
and displacement of the normal L3-L4 disc. We found
stenosis, a condition known as spondylolisthesis.
e
that for all simulations the deformations and
resultant in ammatory process can be con ned to the
displacement are signi cantly higher when the cage is
musculoskeletal tissue or it can advance to the spine and
closed and the lordosis modi ed. us, this experimental
nerve roots with associated neurological de cit. Other
expandable cage, by restoring the natural lordosis could
causes of lumbar back pain can elicit similar symptoms
limit the stresses on the adjacent disc and therefore
but are not related to structural primary degeneration:
prevent progression of the disease and proximal disc
tumors, infection, deformity, post-traumatic sequels,
degeneration.
osteoporosis, systemic and autoimmune diseases,
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
31
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
muscular strain, morbid obesity and pregnancy.
Method
Although spinal arthrodesis was not a new concept, the
posterior lumbar interbody fusion
(PLIF) was
e nite element analysis is a numerical method
introduced by Cloward and represented a signi cant
widely used to obtain solutions to complex equations
evolution in the operative treatment of pathological
that describe or approximate a many physical
spinal disorders [1].
phenomenon. e basis of this method is that a complex
e current literature focuses on minimal invasive
domain can be subdivided into a series of smaller regions
surgery.
is approach is determined by limited muscle
de ned by computable di erential equations, a process
and ligaments derangements rather than skin incisions.
called meshing. By later assembling these sets of
Early favorable results with minimally invasive
equations the whole domain can be determined. In our
transforaminal lumbar interbody fusion (TLIF) as a
study we used ANSYS Workbench 13 software.
method of achieving circumferential lumbar fusion
We started by analyzing the computed tomography
using a unilateral dorsal approach and tubular retractor
(CT) scans of three patients (1-man of 49 years old,
inserted through a muscle-dilating exposure were
2-woman of 55 years old and 3-man of 47 years old) with
reported for refractory mechanical low-back and
chronic low back pain and degenerative modi cations of
radicular pain associated with spondylolisthesis,
the lumbar spine. An average
3D model was then
degenerative disc disease, and recurrent disc herniation
constructed for L3, L4 and L5 vertebra. is was imported
[2].
in the nite element analysis software and material
Low cost TLIF constructs have been proposed
properties were assigned accordingly
(longitudinal
with favorable outcomes. A transforaminal lumbar
elasticity module and Poisson coe cient, Table I).
interbody fusion using unilateral pedicle screws and a
e numerical simulation was performed using the
translaminar screw could reduce the cost of the
Workbench Simulation module for two situations:
posterior implants by almost
50%
[3]. Several
closed and expanded (lordosis restored) cage (Figure 1)
complications have been described with PLIF and
TLIF alike, including intraoperative neurologic injury,
Table I. e mechanical properties
implant migration or subsidence, dural tears, infection,
of the materials used in the analysis
heterotopic ossi cation, BMP-related radiculitis, and
Properties
Young
Poisson
Density
osteolysis [4].
module
coe cient
[kg/mm3]
Material
[MPa]
[-]
We aimed to determine the impact on the adjacent
Ti-6Al-4V
96000
0.36
4.62*10-6
disc of a newly designed expandable TLIF
Austenitic stainless steel
1.93*105
0.31
7.75*10-6
(transforaminal lumbar interbody fusion) cage using
Cortical bone
1.20*105
0.34
3.21*10-6
nite element modeling.
Intervertebral disc
250
0.35
-
A
B
Figure 1. Stages of study model discretization with the cage closed and expanded. A -
Preliminary discretization; B - Further re ning of the study model with the cage expanded
32
Magureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Results
were measured in the elastic deformation and
displacement of the normal L3-L4 disc. e data as
e numerical simulations were performed
well as a t-test comparison using GraphPad can be
comparative for two di erent structures: cage closed
seen in Table II.
and expanded to degrees.
is led to the L4-L5
We have found that for all simulations the
endplates being parallel and with a
4.2 lordosis
deformations and displacement are signi cantly higher
respectively. All other parameters were kept constant.
when the cage is closed and the lordosis modi ed. us,
For each situation we performed 12 simulations aimed
this experimental expandable cage, by restoring the
at reproducing di erent grades of lumbar spine
natural lordosis could limit the stresses on the adjacent
exion. We de ned rotation angles for the L3 vertebra
disc and therefore prevent progression of the disease and
and kept the fused L4-L5 segment rigid. e e ects proximal disc degeneration. (Figure 2,3).
A. Equivalent elastic deformations
B. Total displacement
C. Normal elastic deformations
D. Shear elastic deformations
Figure 2. Results of the numerical analysis with the cage expanded
Figure 3. Selection of the total displacement and elastic deformations respectively,
on a section of the intervertebral disc
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
33
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Table II. Comparative elastic deformations and total displacement during 12 simulations with the cage closed and open
Elastic deformation [mm/mm] Total displacement [mm]
Test
Angular displacement L3 [deg] for 500 N
Cage closed
Cage open Cage closed Cage open
1
1.0
0.150
0.04
0.950
0.47
2
1.8
0.280
0.14
1.730
0.86
3
2.6
0.411
0.195
2.510
1.43
4
3.4
0.520
0.26
3.110
1.64
5
4.2
0.660
0.301
4.070
2.01
6
5.0
0.790
0.39
4.850
2.42
7
5.8
0.920
0.44
5.630
2.94
8
6.6
1.050
0.52
6.400
3.2
9
7.4
1.900
0.61
7.120
3.67
10
8.2
1.300
0.65
7.970
3.98
11
9.0
1.430
0.69
8.750
4.49
12
9.8
1.590
0.78
9.700
4.76
Mean
0.916
0.418
5.232
2.655
SD
0.550
0.236
2.843
1.412
-
P
0.008
0.010
95% CI
0.139-0.857
0.675-4.477
Discussions
e 2009 American Pain Society Clinical Practice
Guideline review on low back pain surgery has
A systematic review of symptomatic degenerative
somewhat nuanced results favoring rehabilitation. For
lumbar disease in patients treated conservatively or by
nonradicular degenerative low back pain fusion is
fusion found higher ODI (Oswestry Disability Index)
slightly to moderately superior to conservative treatment
improvements with spondylolisthesis and degenerative
with less than half experiencing optimal outcomes. For
disc disease compared to chronic low back pain patients,
radiculopathy with herniated disc there is good evidence
regardless of technique [5].
that discectomy is superior over nonoperative therapy.
In addition, for cases of low back pain total disc
For symptomatic spinal stenosis
(with or without
replacements and dynamic stabilizations after
spondylolisthesis) there is also good evidence that
decompression o er only slightly better outcomes
decompressive surgery is superior to conservative
compared to fusion and have not reached the
therapy. Arti cial disc replacement is similarly e ective
improvement seen after total hip or knee arthroplasty
compared to fusion for single level degenerative disc
[6,7]; fusion is still the ‘gold standard’ [6,8] and this
disease and interspinous spacers are superior to
procedure can yield speci c complications such as
nonsurgical therapy for spinal stenosis [7].
adjacent degeneration of the proximal segment. In a
MRI assessment of lumbar intervertebral disc
report of the Swedish spine register (Swespine) spinal
degeneration found that Modic changes correlate with
stenosis is the most common indication for surgery.
the P rrmann grades of disc degeneration but here is no
Disc prosthesis surgery yields comparable results to
correlation between Modic types and surgical outcomes
fusion for disc degenerative pain
[6]. Within the
[9]. Superior results of lumbar total disc arthroplasty
Swedish lumbar spine study group Fritzell et al
were achieved in patients with Modic-1 endplate
performed a prospective randomized comparison of
changes on magnetic resonance images [10].
common surgical techniques used for fusion in patients
e TLIF procedure does not have the potential
with severe chronic low back pain. All surgical
complications described when using combined APF and
techniques were found to comparably reduce pain
PLIF techniques to obtain circumferential fusion. e
(VAS) and decrease disability
(ODI).
e simple
side of facetectomy is chosen according to the subject’s
posterolateral fusion had less radiographic consolidation
symptoms. It can also lead to shorter operative times,
rates, but also less complications and reduced costs
less neurologic injury, and improved overall outcomes
compared to more complex circumferential
(PLIF/
[11]. However, in the case of an isthmic spondylolisthesis,
ALIF) procedures for similar outcomes [8].
the addition of interbody fusion confers superior
34
Magureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
mechanical strength
compared to posterior
6.
Strömqvist B, Fritzell P, Hägg O, Jönsson B, Sandén
instrumentation alone.
is helps maintain the
B; Swedish Society of Spinal Surgeons. Swespine: the
correction but might in uence clinical outcome [12].
Swedish spine register :
e 2012 report. Eur Spine J
Direct anterior/posterior spine fusion yields similar
2013;22(4):953-74.
outcomes to transforaminal lumbar interbody fusion
7.
Chou R, Baisden J, Carragee EJ, Resnick DK, Sha er
(TLIF) in terms of clinical and functional results and
WO, Loeser JD. Surgery for low back pain: a review of
fusion rates. Intra-operative complications are higher in
the evidence for an American Pain Society Clinical
the rst group, mostly due to vein lacerations in the
Practice Guideline. Spine
(Phila Pa
1976)
anterior retroperitoneal approach. On the other hand,
2009;34(10):1094-109.
postoperative complications can be higher in the TLIF
8.
Fritzell P, Hägg O, Wessberg P, Nordwall A; Swedish
group due to graft material extruding against the nerve
Lumbar Spine Study Group. Chronic low back pain
root or wound drainage [13]. In a di erent study, clinical
and fusion: a comparison of three surgical techniques: a
outcomes and nonfusion rate in ALIF were also similar to
prospective multicenter randomized study from the
TLIF. However, the restoration of disc height and lordosis
Swedish lumbar spine study group. Spine (Phila Pa
were superior with ALIF compared to TLIF, while blood
1976) 2002;27(11):1131-41.
loss, operative time, and costs were greater [14].
9.
Yu LP, Qian WW, Yin GY, Ren YX, Hu ZY. MRI
e nite element analysis study found decreased
assessment of lumbar intervertebral disc degeneration
loading and improved posture when the cage was
with lumbar degenerative disease using the P rrmann
expanded. ese could be the premises for improved
grading systems. PLoS One 2012;7(12):e48074.
clinical outcomes as well as decreased incidence of
10.
Blondel B, Tropiano P, Gaudart J, Huang RC, Marnay
adjacent level degeneration after lumbar fusion.
T. Clinical results of lumbar total disc arthroplasty in
Nonetheless, one should always consider all the di erent
accordance with Modic signs, with a 2-year-minimum
approaches as well as dynamic stabilizations and disc
follow-up. Spine (Phila Pa 1976) 2011;36(26):2309-
replacements.
15.
11.
Mura PP, Costaglioli M, Piredda M, Caboni S, Casula
S. TLIF for symptomatic disc degeneration: a
References
retrospective study of 100 patients. Eur Spine J 2011;20
Suppl 1:S57-60.
1. Cloward RB. e treatment of ruptured intervertebral
12.
La Rosa G, Conti A, Cacciola F, Cardali S, La Torre
discs by vertebral body fusion. I. Indications, operative
D, Gambadauro NM, Tomasello F. Pedicle screw
technique, after care. J Neurosurg 1953;10:154-68.
xation for isthmic spondylolisthesis: does posterior
2. Holly LT, Schwender JD, Rouben DP, Foley KT.
lumbar interbody fusion improve outcome over
Minimally invasive transforaminal lumbar interbody
posterolateral fusion? J Neurosurg
2003;99(2
fusion: indications, technique, and complications.
Suppl):143-50.
Neurosurg Focus 2006;20(3):E6.
13.
Faundez AA, Schwender JD, Safriel Y, Gilbert TJ,
3. Sethi A, Lee S, Vaidya R. Transforaminal lumbar
Mehbod AA, Denis F, Transfeldt EE, Wroblewski JM.
interbody fusion using unilateral pedicle screws and a
Clinical and radiological outcome of anterior-posterior
translaminar screw. Eur Spine J 2009;18(3):430-4.
fusion versus transforaminal lumbar interbody fusion for
4. Chrastil J, Patel AA. Complications associated with
symptomatic disc degeneration: a retrospective
posterior and transforaminal lumbar interbody fusion. J
comparative study of
133 patients. Eur Spine J
Am Acad Orthop Surg 2012;20(5):283-91.
2009;18(2):203-11.
5. Carreon LY, Glassman SD, Howard J. Fusion and
14.
Jiang SD, Chen JW, Jiang LS. Which procedure is
nonsurgical treatment for symptomatic lumbar
better for lumbar interbody fusion: anterior lumbar
degenerative disease: a systematic review of Oswestry
interbody fusion or transforaminal lumbar interbody
Disability Index and MOS Short Form-36 outcomes.
fusion? Arch Orthop Trauma Surg 2012;132(9):1259-
Spine J 2008;8(5):747-55.
66.
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
35
Transmittal Letter
In consideration of the Medical Connections/Conexiuni Medicale taking action in reviewing and
editing the above-named Article, e ective upon acceptance of the Article by the Medical Connections/
Conexiuni Medicale (hereinafter re ered to as Med Con), the Autor(s) hereby assign(s) to the Med Con,
its legal representatives, successors and assigns, all publishing rights and each and every other right to the
Article throughout the world, in any language and in any medium, whether as an audiovizual work,
collective work, compilation, derivative work, joint work, literary work, phonorecord, pictorial, graphic or
sulptural work, sound recording, work of visual art, computer program, or any other medium now existing
or which hereafter may come into existence, including the copyright and the right to register the copyright
as well as the right to secure any renewals, reissues, and extensions of any such copyrights in Romania or
in any foreign country. Author(s) may request permission to reuse the manuscript or portions thereof.
Such requests must be in writing and permission by the Med Con shall not be unreasonably withheld. e
Author(s) appoint(s) the Med Con as the Author’s(s’) attorney-in-fact to execute any documents the Med
Con deems necessary to record any of these grants with the Romanian copyright o ce or elsewhere. e
Autor(s) also warrant(s) to the Med Con that the Article is original work of the Author(s) except for
material in the public domain and such excerpts from other works as may be included with the prior
written permission of the copyright owners; that the Article has not been previously published, submitted,
or accepted for publication elsewhere; that the Author(s) have no relationship, nancial or otherwise, with
any manufacturers or distributors of products evaluated in this paper, or alternatively any such relationship
has been disclosed in a footnote to the paper, or the requirement is irrelevant to this paper.
Manuscript Title: ___________________________________________________________
Name:
Signature/Date:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Please fax this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
ORIGINAL ARTICLES
APPENDECTOMY IN OBESE PEOPLE. CLASSIC OR LAPAROSCOPIC
APPROACH?
Marius Sfîrlea1, Adrian Maghiar1, Teodor Maghiar2, Dan Ciurtin1, Codru a Macovei1, George Dejeu1,
Ciprian Borza2, Daniela Berdea3, Daniela Rahotă4
1General Surgery Clinic, 2Urology Department, 3Radiology and Imaging Section, 4Hygiene Department, Oradea “Pelican”
Hospital, a liated at the Faculty of Medicine and Pharmacy, Oradea University, Romania, Surgery Clinic 1 of the
Oradea Regional Clinical Hospital and the Surgery Clinic of the Oradea “Pelican” Clinical Hospital
Address for correspondence:
Sfîrlea Marius
Pelican Hospital, 2 Corneliu Coposu St., Oradea, Bihor
Email: s rleamarius@yahoo.com
Received: 25.08.2013
Accepted: 28.02.2014
Med Con March 2014, Vol 9, No 1, 37-41
Abstract
Results:
e mean duration of the surgical
intervention was relatively longer for the laparoscopic
Obese people represent a special category of patients
intervention (51 compared to 48 minutes). e early
with more frequent secondary diseases and higher
infectious complications were less frequent in the
anaesthetic risk, in comparison with normal body
laparoscopic group
(22.7% vs.
73.3%).
e main
weight patients. From the surgical point of view, the
complication was the deep abscess, one case in each of
operation manoeuvres are rendered more di cult by the
the two subsets of patients. e need for post-operative
thickness of the abdominal wall and the large volume of
analgesics was lower
(90% vs. 42%) for the mini-
peritoneal fat covering the surgical area. e introduction
invasive operated patients. e hospital stay and charges
of the mini-invasive laparoscopic techniques o er new
were lower in the group of mini-invasive operated
surgical possibilities with obvious advantages compared
patients than in the subset of those operated through
to the classic ones. is retrospective study was made on
the classic approach.
two groups of obese patients who underwent
Conclusion: Laparoscopic appendectomy in obese
appendectomy, one through the classical procedure and
people is a viable alternative with the possibility of
the other one laparoscopically.
e intra-operative
conversion in di cult surgical situations.
aspects and the post-operative evolution were compared
Keywords: Classic appendectomy, laparoscopic
in order to appreciate the optimal treatment variant.
appendectomy, appendicitis, obesity
Material and Methods: During the period 2004-
2013, classic appendectomy was performed on a group
Introduction
of 49 obese patients and laparoscopic appendectomy
was performed on 24 obese patients. We have analysed
A priori acute appendicitis is considered a simple
comparatively the duration of the surgery, the post-
intervention in the abdominal surgery, being performed
operative pain, the post-operative complications,
by more than one century [1] through the classical
hospital stay and charges, in order to highlight the
technique, through a McBurney incision, with good
potential bene ts of laparoscopy in comparison with the
results. In the last 30 years the wide introduction on the
open approach in appendicitis in obese people.
minimal invasive laparoscopic techniques o ered a new
Appendectomy in Obese People. Classic or Laparoscopic Approach?
37
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
approach for the treatment of the appendicitis a ections
records.
e data of the patients were used with their
through the laparoscopic appendectomy. e laparoscopic
consent and they were treated con dentially.
surgery imposes as e cient in the pathologies of the
e statistic analysis was made with the EPIINFO
bladder, the colon, the rectum, gynaecological and various
6.0 application and the Student test.
hernias. In what regards appendectomy, we observed a
certain resistance from the surgeons, at least in Romania
Results
[2]. Obese patients represent a special category apart from
the normal-weight ones, presenting the problems of
General data
frequent secondary diseases, such as cardiovascular and
e sex and age group repartition was similar in the
respiratory a ections or diabetes mellitus.
e associated
two subsets with a slight predominance of the women
anaesthetic risk is much higher, requiring a more serious
and the second and third decades of life. e prevalence
preoperative preparation [3]. From the surgical point of
of the associated diseases was 28.6% in the group with
view in the case of obese patients the operation manoeuvres
classical intervention, respectively 33.3% in that with
are disturbed by the thickness of the abdominal wall which
laparoscopic intervention (p=0.319), (Table I).
requires longer incisions in the open surgery and by the
e anaesthesia used in the subset with classic
high volumes of peritoneal fat covering the surgery area
intervention was rachidian in 31 cases (63.3%) and
[4].
ese obstacles determined di culties in the
general through intubation in 18 cases (36.7%), while
laparoscopic surgery in the introduction of the rst trocar,
in the laparoscopic intervention only general anaesthesia
the infusion of the pneumoperitoneum, the ventilation of
was used (100.0%) (Table II).
the patient after the positioning in Trendelenburg and the
e approach method for the patients operated
view obstructed by the epiploic fat [5,6].
open was the widened McBurney incision in 43 cases
e purpose of our study was to highlight the
and median incision in three other cases associated with
potential bene ts of laparoscopy in comparison with the
a broken ectopic pregnancy, an intestinal occlusion
open approach in the appendectomy in obese people,
through adherences and a pelviperitonitis. In the second
relying on the experience accumulated in the last 5 years
subset laparoscopic appendectomy with three trochars
in our service, by the introduction of the laparoscopic
was performed in
23 cases and in one case SILS
approach in the acute appendicitis, with the possibility
appendectomy with sole trans-umbilical mini-invasive
of easy conversion to the open surgery in the complicated
approach was performed on one female patient.
cases.
Material and Methods
Table I. Case distribution according
to the associated diseases
Among the appendicectomized patients we selected
Classic
Laparoscopic
Associated diseases
the obese ones with a body mass index (BMI) over 30,
N°
% N°
%
operated between 2004-2013 by the same surgical sta .
Cardiovascular diseases
10
20.4
4
16.7
We selected two subsets: One made of
49 patients
Diabetes mellitus
2
4.1
1
4.2
operated through the open approach and 24 patients
Respiratory diseases
8
16.3
5
20.8
operated laparoscopically for whom we compared the
Total
14
28.6
8
33.3
duration of the operation, the anaesthesia type, the
amount of major analgesics post-operative, the post-
Table II. Case distribution according
operative complications, the hospital stay and charges. As
to the type of anaesthesia
a surgical intent, the laparoscopic subset initially included
38 patients, but in 14 of them (36.8%) we decided the
Classic
Laparoscopic
Anaesthesia
conversion to the open approach due to the dysfunctions
N°
% N°
%
related to the laparoscopic device or the surgical technical
Rachidian
31
63.3
0
0.00
di culties.
ey were included in the group of those
General with intubation
18
36.7
24
100.0
operated surgically. Seven of these converted patients had
a gangrenous appendicitis or peritonitis.
Table III. Mean duration of the intervention
e data were collected through the analysis of the
operation records of the patients, the study of the
Classic
Laparoscopic
operation protocols, the computer database from the
Limits
31-150 min
30-90 min
hospitals and the exam of the intra-operatory video
Mean duration
48±22 min
51±25 min
38
Sfîrlea et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
e duration of the intervention was between 31-
modi cations
(46.2% and
50.0% respectively)
150 minutes in the classical operation, resulting a mean
(p=0.447) (Table V).
of 48 minutes and between 30-90 minutes resulting a
Gynaecological associated pathologies, mesenteric
mean of 51 minutes in the laparoscopic intervention
lymphadenitis, acute cholecystitis or intestinal occlusion
(Table III).
with adherences were present in 30.8% of the cases with
In the rst day after the surgery opiates
classic intervention, respectively
50.0% of the
administration happened in 44 cases in the subset with
laparoscopic one (p<0.001). Finally, appendectomy was
classical intervention (89.8%) and in 10 cases in the
applied in
45 cases from the subset with classic
laparoscopic one (41.7%).
intervention (91.8%) and in 22 cases from the one with
Morphopathological analysis
laparoscopic intervention (91.7%).
Among the con rmed cases of acute appendicitis
Complications
(36 of the classic intervention groups and 20 of those
Early infectious complications were signi cantly
with laparoscopic ones), most of them were catarrhal or
more frequent in the group with classic appendectomy
phlegmonous (55.6 and 65.0% respectively) (p=0.046).
compared to the laparoscopic method (73.3% vs. 22.7%)
Acute gangrenous appendicitis was present in
(p<0.001). e most frequent early complication was the
25.0% of the cases and 15.0% respectively (p=0.005),
infection of the wound, found in 68.9% of the patients
appendicular peritonitis in
13.9% of the cases,
with classic appendectomy and in 18.3=2% of those with
respectively 10.0% (p=0.195) and the periappendicular
laparoscopic appendectomy (p<0.001) (Table VI).
block with abscess was present in 5.6% of cases and
In each group of obese patients there was a
10.0% respectively (p=0.142). From the statistic point
complicated case with intraperitoneal abscess which
of view there are signi cant di erences between the two
responded well to conservation treatment with antibiotics.
groups in what regards the type of acute appendicitis
One patient operated with the classic method showed 5th
(p=0.009) (Table IV).
day peritonitis which was resolved conservatively.
e diagnostic of acute appendicitis was not
Other early post-operative complications were
con rmed in 13 cases (26.5%) from the group with
reported in 26.7% of the cases with classic appendectomy
classic intervention and 4 cases (16.7%) from the subset
and in 18.1% of those with laparoscopic appendectomy
with laparoscopic intervention. Among these most of
(p=0.026). In the groups with classic appendectomy
them had a healthy appendix, without macroscopic
most of the cases were early ileus (4 cases - 8.9%) of
Table IV. e case distribution according
Table VI. e case distribution according
to the morphopathological type of the appendicitis
to the early infectious complications
Classic
Laparoscopic
Classic
Laparoscopic
Morphopathology
Early complications
N°
% N°
%
N°
% N°
%
Catarrhal or phlegmonous
20
55.6
13
65.0
Wound infections
31
68.9
4
18.2
Gangrenous
9
25.0
3
15.0
Deep abscess
1
2.2
1
4.5
Appendicular peritonitis
5
13.9
2
10.0
Periappendicular block
5th day peritonitis
1
2.2
0
0.0
2
5.6
2
10.0
with abscess
Total
33
73.3
5
22.7
Total
36
100.0
20
100.0
Table V. e distribution of the diagnostic in the case in
Table VII. e case distribution according
which the appendicitis was in rmed during the operation
to other early complications
Classic
Laparoscopic
Other early
Classic
Laparoscopic
N°
% N°
%
complications
N°
% N°
%
Healthy appendix
6
46.2
2
50.0
Bleeding
1
2.2
0
0.0
Gynaecological pathology
4
30.8
2
50.0
Early ileus
4
8.9
1
4.5
Occlusion / adherences
1
7.7
0.0
Evisceration
1
2.2
0
0.0
Cholecystitis
1
7.7
0.0
Respiratory infections
3
6.7
1
4.5
Mesenteric lymphadenitis
1
7.7
0.0
Urinary infections
3
6,7
2
9.1
Total
13
100.0
4
100.0
Total
12
26.7
4
18.1
Appendectomy in Obese People. Classic or Laparoscopic Approach?
39
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
which 3 patients were cured conservatively and in the
Post-operative pain assessed through the need of
case of one patient there was another intervention
opiate medicines administered after the surgery was
performing a median laparotomy and adhesiolysis. A
obviously more reduced in the case of patients operated
single case in the group of patients with laparoscopic
laparoscopically, clearly due to the lower parietal trauma.
operated appendectomy showed a post-operative ileus
Among the early complications, the most studied
cured under conservatory treatment.
and frequent in the literature are the early infectious
One of the cases operated classically showed a
ones which can be super cial, within the wound or deep
haemorrhage in the abdominal wall exteriorized by
into the peritoneum. In obese people, the more
drain requiring the reintervention on the McBurney
abundant fatty tissue, with a more reduced
scar. A patient operated through median approach
vascularization and a reduced capacity of immune
showed an evisceration at the lower pole of the wound
defence represents the election place for the seeding of
for which the reintervention under general anaesthesia
the germs from the peritoneum thus leading to post-
was necessary (Table VII).
operative infections.
e more reduced length of the
e late complications were observed in the cases
incisions in the adipose wall and its more reduced
presented for control in our clinic which required
trauma through the use of trocars as well as the lack of
surgical treatment.
direct contact with the infected appendix during the
In the group with classic appendectomy, there were
manoeuvres for its extraction explain the more reduced
6 cases with late complications (13.3%), of which 4
frequency of the parietal infections
(73.3% versus
cases of eventration (8.9%), 3 on the McBurney incision
22.7%). ere was a case of deep post-operative abscess
and one on median laparotomy. Other 2 cases required
and one case of 5th day peritonitis which were resolved
the reintervention on medial line for the adherence
conservatively.
ese results are similar to those
syndrome
(4.4%). In the subset with laparoscopic
described in literature [6,7].
appendectomy there was a single case with late
e average hospital stay in patients with classic
complication, a patient with post-operative adherence
intervention was almost double compared to the
syndrome for whom laparoscopic adhesiolysis was
patients with laparoscopic intervention (6.2 days vs. 3.3
performed (4.5%) (p<0.001) (Table VIII).
days) (p<0,001). is thing is also due to the apparition
of the post-operative early complications signi cantly
Table VIII. Case distribution according
more frequent in the case of the classic intervention, but
to the late complications
also the slower post-operative recovery of the obese
Classic
Laparoscopic
patients operated though laparotomy.
Late complications
We have calculated the costs considering the average
N°
% N°
%
days of hospitalization of the patients in the two obese
Eventration
4
8.9
0
0.0
groups as well as the consumption of medicines,
Adherence syndrome
2
4.4
0
0.0
imagistic investigations and the various types of
Occlusion/clamps
0
0.0
1
4.5
anaesthetic use.
Total
6
13.3
1
4.5
Contrary to the results in the literature [8,9], the
mean cost / case was higher in the subset with classic
Discussions
interventions (2,253 lei vs. 1,955 lei), di erence due
mainly to the complications which required more days
Some of the results obtained through the present
of recovery in the ICU and complex medicine, but also
study require a special attention. Hence, approximately
a higher number of hospital days.
one third of the patients, most of them bellow 40 years
We must mention that we did not introduce in the
presented an associated cardiac, respiratory pathology or
calculation the amortization of the laparoscopy tools
diabetes mellitus, showing the di culties related to the
which represent an important nancial weight and the
surgery in obese people. Another important aspect is
cost of the consumable materials was insigni cant. We did
related to the duration of the surgical intervention,
not use endoscopic staplers for the ligature of the appendix
where there were no signi cant di erences (48 vs. 51
and its mesentery, but endoloops pre-knotted by us with
minutes), this being explained through longer times
Biocryl 2-0 thread while for the extraction of the appendix
necessary for laparotomy
(in
3 cases median sub-
we improvised endobags from a surgical glove.
umbilical) and for the closing of the wall in obese people
Laparoscopic appendectomy in obese people is
in comparison with those necessary for the introduction
associated with fewer post-operative complications than
of trochars.
the open one, but the rate of deep post-operative abscesses
40
Sfîrlea et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
is a little higher (45% vs. 2.2%), results which comply
2.
Nicolau A E. Apendicectomia laparoscopică Chirurgia
with most of the published studies. e average operation
2011;106:495-503.
time is insigni cantly higher for the patients with
3.
Dority J, Hassan ZU, Chau D. Anesthetic implications
laparoscopy (51 vs. 48 minutes). e average hospital stay
of obesity in the surgical patient. Clin Colon Rectal
was more reduced compared to the one of the patients
Surg. 2011 ;24(4):222-8.
with open surgery
(6.2 vs.
3.3 days).
rough the
4.
Mason RJ, Mason AJ. Open-close case? New data on
exclusion of the amortization expenses of the laparoscopy
appendectomy in an obese patient cohort. Expert Rev
devices, the average hospital cost was more favourable for
Gastroenterol Hepatol 2013;7(1):1-3.
the laparoscopic surgeries. For the interpretation of these
5.
Corneille MG, Steigelman MB, Myers JG, Jundt J,
results we must take into account the fact that 14 of the
Dent DL et al. Laparoscopic appendectomy is superior
patients in which we tried the laparoscopic approach were
to open appendectomy in obese patients. Am J Surg
included in the subset of 49 patients operated through
2007;194(6):877-80.
the classic method due to the intra-op technical
6.
Mason RJ, Moazzez A, Moroney JR, Katkhouda N.
di culties, 7 of them su ered gangrenous or perforated
Laparoscopic vs open appendectomy in obese patients:
appendicitis with severe periapendicular in ammations.
outcomes using the American College of Surgeons
National Surgical Quality Improvement Program
Conclusion
database. J. Am Coll Surg
2012;215(1),
88-99;
discussion 99.
Laparoscopic appendectomy in obese people
7.
Gaszynski T.
e e ect of pneumoperitoneum on
represents a convenient surgical variant for the patients
haemodynamic parameters in morbidly obese patients.
considering the possibility of conversion to classic
Anestezjol Intens Ter 2011;43(3):148-52.
surgery in the complicated cases.
8.
Gorenoi V, Dintsios CM, Schönermark MP, Hagen
A. Laparoscopic vs. open appendectomy: systematic
review of medical e cacy and health economic analysis.
References
GMS Health Technol Assess 2007;2:Doc22.
9.
Kehagias I, Karamanakos SN, Panagiotopoulos S,
1. McBurney C. e incision made in the abdominal wall
Panagopoulos K, Kalfarentzos F. Laparoscopic versus
in cases of appendicitis, with a description of a new
open appendectomy: which way to go? World J
method of operation. Ann Surg 1894;20:38-43.
Gastroenterol 2008;14(31):4909-14.
Appendectomy in Obese People. Classic or Laparoscopic Approach?
41
Grocery Store, early twentieth century,
nowadays at corner of Horia St. with Ion IC Brătianu Blvd.
(Băcănie, începutul secolului XX,
în prezent intersec ia străzii Horea cu bulevardul Ion IC Brătianu)
Foto 2: Corso, “at the Electric Clock”, Center of Satu Mare City
(Corso, „la ceasul electric”, Centrul oraşului Satu Mare)
ORIGINAL ARTICLES
INCIDENCE OF ATYPICAL LYMPHATIC DRAINAGE IN PATIENTS
WITH MALIGNANT MELANOMA
Florin Suru, Adrian Maghiar
Department of Surgery, Faculty of Medicine and Pharmacy, Oradea University
Address for correspondence:
Florin Suru
Phone: 0744760240
E-mail:
_suru@yahoo.com
Received: 15.01.2014
Accepted: 28.02.2014
Med Con March 2014, Vol 9, No 1, 43-47
Abstract
patients for lower respectively upper limbs.
e overall
incidence of atypical lymphatic drainage was 18.83%
Regional lymph nodes draining the primary
(29 out of 154 patients).
melanoma are the most common initial metastatic sites in
Conclusion: Atypical drainage is most frequently in
patients with stage I and II disease. erefore, the precise
melanomas of the head and neck, followed by those of
location and drainage lymph node staging are crucial in
the trunk. Preoperative lymphoscintigraphy drainage
the treatment of these patients. Lymphoscintigraphy
allows de ning individual, personal patterns, largely
studies have proved variability in lymphatic drainage
contributing to the success of sentinel lymph node
patterns in di erent regions of the primary melanoma.
selective dissection.
Objective: Correlation of lymphatic drainage
Keywords: malignant melanoma, lymphoscintigrafy,
patterns from the following three sources: preoperative
sentinel lymph node, atypical lymphatic drainage
clinical prediction based on the anatomical location of
the primary tumor, lymph drainage pattern determined
Introduction
by preoperative lymphoscintigraphy and SLN
identi cation during surgery.
Regional lymph nodes draining the primary
Materials
and
Methods:
Preoperative
melanoma are the most common initial metastatic sites
lymphoscintigraphy was performed on
154 patients,
in patients with stage I and II disease [1]. erefore, the
hospitalized and operated in the Department of
precise location and drainage lymph node staging are
Oncological Surgery of the Municipal Hospital Timişoara,
crucial in the treatment of these patients.
with various stages of primary malignant melanoma.
Traditionally, the draining lymph nodes were
Results: Preoperative lymphoscintigraphy identi ed
dissected for prophylactic purposes. Basins dissected
at least one SLN in all patients included in the study.
during elective lymph node dissection were based on the
Among patients with head and neck melanomas - 6
colloid anatomical patterns of lymphatic drainage from
(33.33%) of the 18 patients - had at least one SLN
the skin on dead bodies described by Sappey [2] and
outside clinically anticipated areas. Discordance for
modi ed by Sugarbaker and McBride [3] based on
melanoma of the trunk was seen in 16 (24.61%) of 65
clinical patterns.
cases. Melanomas on the extremities showed atypical
e development of the technique of selective
drainage to SLN 4 (16.66%) of 24 and 3 (6.38%) of 47
sentinel lymph node dissection (SSLN) for patients with
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
43
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
melanoma is a major progress in their treatment [4].
lymphoscintigraphy were identi ed. Patients under 18
Many studies have established that the SLN condition
and pregnant women were excluded.
certainly predicts the nodal basin condition [5].
is
A brief description of the lymphoscintigraphy
minimally invasive technique allows the SLN
technique: technetium Tc 99m (99mTc) colloidal sulfur
pathological evaluation. When the results of the
ltered through a 22 µm lter was injected intradermally
pathological evaluation are negative lymph nodes basin
around the primary tumor or the post-biopsy scar. With
dissection is no longer required as the evaluations for
a dual head gamma camera (ADA Vertex) dynamic
these are negative in more than 95% of the cases [6].
images are immediately obtained in order to evaluate
However, the precision of the SSLND technique depends
the radiotracer uptake in the lymph vessels. Delayed
on the reliability of the preoperative lymphoscintigraphy
images are recorded from 20 minutes to 2 hours in order
localization of the SLN. Lymphoscintigraphy proved to
to detect all the basins predisposed to metastasis spread
be an excellent predictor of lymphatic drainage from the
and to study the radiocoloidale substance uptake by
primary melanoma based on nodal recurrences, as
viewing the trace in the liver. SLN localization is marked
demonstrated by long-term monitoring [7].
on skin with a dye (non-radioactive ink).
Early lymphoscintigraphy studies have shown the
Prior to surgery lymphazurin blue - Bleu Patent
variability of lymphatic drainage patterns in di erent
(1% in an aqueous solution) - is injected around the
regions of the primary malignant melanoma. Although the
primary melanoma or around the site where the biopsy
head and neck region appears to show the greatest variability
was performed (about 4 points).
[8] the chest region also shows signi cant variations [9,10],
Sentinel lymph node selective dissection procedure
especially for melanoma arising in the midline and in the
is associated with a wide local excision of the primary
vicinity of the Sappey’s line. Drainage from melanoma the
tumor. Using a manual gamma probe
(Neoprobe
extremities were considered to be less variable.
Corporation, Dublin, Ohio) lymph nodes with high
Preoperative and intraoperative lymphoscintigraphy
gamma-ray emission are localized. For an accurate SLN
through SLN mapping may be a preferred alternative to
identi cation the high rates of signal node-background
traditional elective node dissection based on anatomical
[12] or the blue staning of the lymph nodes.
preoperative
predictions
[11].
Preoperative
Clinical prediction of lymphatic drainage basins
lymphoscintigraphy will accurately identify the nodal basin
localization from primary tumor site was made according
drainage, and then the intraoperative SLN mapping will
to standard patterns of drainage. For the legs, lymphatic
facilitate SSLND for a proper staging of the nodal basin,
drainage from the cutaneous area is expected in the inguinal
thus saving about 80% of patients with malignant melanoma
area (femoral area). Drainage in the popliteal area was
from an unnecessary elective lymphatic dissection [4].
considered atypical. For the upper limbs the only presumed
area was the axillary area. Drainage of epitrochlear or
Objective of the study
supraclavicular areas was considered atypical.
For patients with melanomas of the trunk,
is study evaluates the incidence of lymphatic
lymphatic drainage is expected in the nearest inguinal or
drainage, inconsistent with classical anatomical patterns,
axillary area [2,3]. If the primary tumor was located less
in patients with invasive malignant melanoma. In this
than 2.5 cm from the midline, drainage can occur on
respect, the results of the lymphatic drainage mapping
any part or bilaterally, not being considered atypical.
by preoperative and intraoperative lymphoscintigraphy
Similarly, for the primary melanoma located less than
were compared to traditional anatomical patterns as
2.5 cm from Sappey’s line drainage may appear in the
well as with those with clinical predictions.
ipsilateral areas, inguinal or axillary, or both. For
example, a primary tumor localized around the navel or
Materials and methods
in the area L2 may drain in any inguinal or axillary
basins combination without being considered atypical.
Patients for this observational, retrospective and
For patients with primary malignant melanoma of the
prospective, cohort study were selected from patients
head or neck, aberrant drainage detection algorithm was
hospitalized in the Department of Surgical Oncology
based directly on the pattern illustrated by O’Brien et al.
from Timişoara Municipal Hospital for invasive
[8]. Primary lesions were classi ed by location in 10 regions
malignant melanoma during 2001-2013.
of the head and neck. e identi ed drainage areas were:
All patients who underwent primary tumor biopsy
parotid (area 1), submandibular or submental triangle (area
(surface biopsy, needle biopsy, excisional or incisional
2), upper jugular (area 3), middle jugular (area 4), lower
biopsy) and selective SLN dissection after
jugular (area 5), posterior triangle (area 6) and occipital
44
Suru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
area
(area
7). If a primary tumor revealed lymphatic
Table I. e drainage areas corresponding
drainage outside of the prediction area, that drainage was
to the regions of the primary tumor
considered atypical. Table I shows the drainage areas
Expected drainage
Primary tumor localization
corresponding to the regions of the primary tumor.
area
e criteria pursued in this study were the number
Anterior scalp
1-4
and localization of SLN for each patient and its
Coronal sclap (5 cm band)
1-6
comparison with the anatomic drainage pattern
Posterior scalp
2-5.7
Face
1-4
previously described. In addition to these data there also
Ear
1-6
were noted: age, sex, Clark level of invasion, Breslow
Anterior superior neck
1-5
scale thickness, and histopathological result of SLN.
Coronal neck (5 cm band)
1-6
Upper posterior neck
2-5.7
Results
Anterior inferior neck
3-5
Lower posterior neck
3-5
e number of patients who met the inclusion and
exclusion criteria of this study was 154. 60 of them were
men (39%) and 94 women (61%), with a median age of
Table II. e number of SLN intraoperatively identi ed
53.9 years (SD=13.45).
Number of
No. of
Percentage
p*
Medium thickness on Breslow scale was 2.53 mm
identi ed SLN patients
(%)
(SD=1.43), with a median Clark level of invasion of 3
0
5
3.2%
(IC95%=3-4).
1
115
74.7%
All patients underwent lymphoscintigraphy, being
2
26
16.9%
<0.0001
identi ed at least one preoperative SLN basin.
e
3
4
2.6%
number of SLN intraoperatively identi ed has evolved
4
4
2.6%
as is shown in Table II.
* chi-square test
Table III. e situations of atypia, analyzing the results of lymphoscintigraphy
together with the predictive lymphatic drainage patterns
Primary tumor localization and lymphatic drainage pattern
Atypia cause
Number of cases
Head and neck (n=18)
Standard
No
12
Drainage in an area noncordant with the expected area*
Atypical drainage
6
Trunk (n=65)
Standard
No
49
Contralateral axillary
Drainage over the the midline
6
Contralateral inguinal
Drainage over the the midline
1
Anterior and/or posterior cervical
Atypical drainage
2
Supraclavicular
Atypical drainage
3
oracic wall
Atypical drainage
2
Lower lumbar
Atypical drainage
1
Posterior triangle
Atypical drainage
1
Upper extremities (n=24)
Axillary
No
20
Axillary and epitrochlear
Additional basin
1
Axillary and supraclavicular
Additional basin
1
Axillary and subclavicular
Additional basin
1
Only supraclavicular
Atypical drainage
1
Lower extremities (n=47)
Inguinal
No
44
Inguinal and popliteal
Additional basin
3
* see Table I
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
45
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
In return the overall incidence and the distribution
by body regions of the cases of atypical lymphatic
drainage from the primary melanoma were comparable
to data from the literature [14].
Conclusions
As emerges from this study as well, preoperative
lymphoscintigraphy is an essential condition for the
selective SLN dissection.
For patients with extremities
melanoma,
lymphoscintigraphy allows the rare identi cation of
Figure 1. e incidence of atypical lymphatic drainage
drainage to other basins than the axillary and inguinal
ones. For primary tumors localized on the trunk, standard
Regarding the histopathological result, from the
drainage patterns may include ipsilateral or bilateral basins
total of
154 patients
61 (39.6%) was found with
and the atypical drainage may involve nodes in transition
micrometastases in the dissected SLN.
ese patients
or unusual drainage ganglions. For head and neck drainage
underwent extensive neck dissection.
is highly variable, and lymphoscintigraphy provides an
Analyzing the results of lymphoscintigraphy
important weapon meant to guide the surgeon to the areas
together with the predictive lymphatic drainage
that drain a particular primary melanoma.
patterns, the situations of atypia were noted in Table III.
Preoperative lymphoscintigraphy allows the
e incidence of atypical drainage respects the
de nition of individual, personal drainage patterns,
literature data, being the most frequent on the head, neck
thus largely contributing to the success of selective
and trunk areas (p=0.0330, chi-square test), Figure 1.
sentinel lymph node dissection.
e overall incidence of atypical lymph drainage
was 18.83% (29 patients out of 154 cases).
References
Discussions
1.
Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic
Given the values presented above, it can be seen
factor analysis of 17,600 melanoma patients: validation
that, for most patients the number of intraoperatively
of the American Joint Committee on Cancer melanoma
identi ed SLN has been 1 or 2. And prevalence of
staging system. J Clin Oncol 2001;19:3622-3634.
malignant melanoma micrometastasis was nearly 40%.
2.
Sappey MPC. Anatomie, Physiologie, Pathologie des
Comparing the frequency of atypia for various sites
Vaisseaux Lymphatiques Conside´re´s Chez l’Homme et
of primary melanoma, it is established the predominance
les Verte´bre´s. Paris, France: DeLahaye A, Lecrosnier
of these anomalies in primary tumors on the trunk,
E; 18[74]85.
head and neck consisting of more than 55% of atypical
3.
Sugarbaker EV, McBride CM. Melanoma of the trunk:
drainage cases.
the results of surgical excision and anatomic guidelines
e high value of the overall incidence of atypical
for predicting nodal metastasis. Surgery 1976;80:22-
lymphatic drainage gives lymphoscintigraphy a special
30.
importance in SLN mapping.
4.
Leong SPL. e role of sentinel lymph node in human
is analysis clearly shows that without accurate
solid cancer. In: Devita VT, Hellman S, Rosenberg
lymphoscintigraphy and mapping of individualized
SA, eds. PPO Updates. Philadelphia, Pa: Lippincott-
lymphatic drainage for each patient we risk as the true
Raven Publishers; 1998:1-12.
SLN may not be identi ed and dissected.
5.
Morton DL, ompson JF, Cochran AJ, et al. Sentinel
ese results are closer to the observations in the
node biopsy or nodal observation in melanoma. N Engl
specialized studies.
e incidence of positive lymph
J Med 2006;355:1307-17.
nodes in the histopathological examination is slightly
6.
Clary BM, Brady MS, Lewis JJ, Coit DG. Sentinel
higher than in similar studies [13] which are probably
lymph node biopsy in the management of patients with
explained by the fact that patients had a more advanced
primary cutaneous melanoma: review of a large single-
stage of disease at the time of hospitalization compared
institutional experience with an emphasis on recurrence.
to the groups studied in the literature.
Ann Surg 2001;233:250-8.
46
Suru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
7. Berger D, Feig B, Podolo D, et al. Lymphoscintigraphy
11.
ompson JF, Uren RF, Shaw HM, et al. Location of
as a predictor of lymphatic drainage from cutaneous
sentinal lymph nodes in patients with cutaneous
melanoma. Ann Surg Oncol 2004;4:247-51.
melanoma: new insights into lymphatic anatomy. J Am
8. O’Brien CJ, Uren RF, ompson JF, et al. Prediction
Coll Surg 1999;189:195-206.
of potential metastatic sites in cutaneous head and neck
12. Albertini JJ, Cruse WC, Rapaport D, et al.
melanoma using lymphoscintigraphy. Am J Surg
Intraoperative
radiolymphoscintigraphy
improves
1995;170:461-6.
sentinel lymph node identi cation in melanoma. Ann
9. Uren DF, Howman-Giles RB, Shaw HM, ompson
Surg 1996;223:217-24.
JF, McCarthy WH. Lymphoscintigraphy in high risk
13. Karim RZ, Scolyer RA, Li W, et al. False negative
melanoma of the trunk: predicting draining node groups,
sentinel lymph node biopsies in melanoma may result
de ning lymphatic channels and locating the sentinel
from de ciencies in nuclear medicine, surgery, or
node. J Nucl Med 1993;34:1435-40.
pathology. Ann Surg 2008;247:1003-10.
10. Lamki LM, Logic JR. De ning lymphatic drainage
14. Gershenwald JE, ompson W, Mans eld PF, et al.
patterns with cutaneous lymphoscintigraphy. In: Balch
Multi-institutional melanoma lymphatic mapping
CM, Houghton AN, MiltonGW,Sober AJ, Soong SJ,
experience: the prognostic value of sentinel lymph node
eds. Cutaneous Melanoma. 2nd ed. Philadelphia, Pa:
status in 612 stage I or II melanoma patients. J Clin
Williams&Wilkins; 1992:367-75.
Oncol 1999;17:976-83.
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
47
Liberty Square, the beginning of Alexandru Ioan Cuza St.
(Pia a Libertă ii, începutul străzii Alexandru Ioan Cuza)
Dacia, former Pannonia Hotel
(Hotelul Dacia, fost Pannonia)
CASE PRESENTATION
NEPHROTIC SYNDROME AND ACUTE RENAL FAILURE CAUSED BY
CHRONIC LYMPHOCYTIC LEUKEMIA. CASE REPORT AND REVIEW
OF THE LITERATURE
Boris Solun1, Dana Marcoviciu1, Yulia Belnik1, Avraham Sendovski1, Dror Dicker1, Ana Tovar2
Departments of
1Internal Medicine D and 2Pathology, Rabin Medical Center, Petah Tikva, a liated to the Sackler
School of Medicine, Tel Aviv University, Tel Aviv, Israel
Address for correspondence:
Dr. Boris Solun, MD
Department of Internal Medicine D
Rabin Medical Center - Hasharon Hospital
7 Keren Kayemet St., Petach Tikva 49100, Israel
Phone: 972-3- 9372426, Fax: 972-3-9372427
E-mail: bsolun@gmail.com
Received: 14.01.2014
Accepted: 15.02.2014
Med Con March 2014, Vol 9, No 1, 49-54
Abstract
of CLL, occurring as a consequence of hypogamma
globulinemia and treatment with immunosuppressant
Renal involvement in chronic lymphocytic leukemia
and monoclonal antibodies.
(CLL) is not unusual and is typically due to kidney
Keywords: Chronic lymphocytic leukemia,
in ltration by leukemic cells. However, CLL associated
nephrotic syndrome, treatment
with proteinuria due to glomerular involvement with
Abbreviations: CLL, chronic lymphocytic
nephrotic syndrome occurs in only 1%-2% of patients.
leukemia;
MPGN,
membranoproliferative
e rarity of glomerulopathy in this setting suggests
glomerulonephritis
that tumor cells may have certain properties leading to
the development of glomerulonephritis. e aim of this
Introduction
report was to describe a patient with CLL, acute renal
failure, nephrotic syndrome, and cryoglobulinemia.
Chronic lymphocytic leukemia
(CLL) may be
Bone marrow biopsy revealed di use spread of a large
complicated by acute renal failure, usually as a
number of small lymphocytes, compatible with the
consequence of kidney in ltration by leukemic cells.
diagnosis of CLL. Renal biopsy demonstrated a
However, direct tumor in ltration and B-cell
membranoproliferative glomerulonephritis pattern,
proliferation with further glomerular involvement
with exudative and necrotizing lesions compatible with
presenting as proteinuria or nephrotic syndrome occurs
cryoglobulinemia. Combined treatment with rituximab,
in only 1% to 2% of patients. is association was rst
dexamethasone, and chlorambucil led to an
described by Scott in 1957 [1,2].
e most common
improvement in both the renal function and proteinuria,
lesion in nephrotic syndrome is membranoproliferative
supporting the para neoplastic nature of the glomerular
glomerulonephritis
(MPGN) [3]. Cryoglobulinemia,
involvement.
e patient died of complications of
predominantly type 1, has been implicated in the link
pneumonia several months later. Infections, usually of
between MPGN and CLL
[4].
e rarity of
bacterial origin, are a major complication of management
glomerulopathy in patients with CLL may indicate a
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
49
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
para neoplastic syndrome. is assumption is supported
count and thrombocyte count were within normal
by the substantial improvement of both diseases with
limits. Blood creatinine was
2.7mg/dl (0.8 mg/dl 5
chemotherapy [5,6]. e aim of the present report was
months before), urea 145.8 mg/dl, sodium 142 mEq/L,
to describe a patient with CLL, acute renal failure,
potassium 7.19 mEq/L, chloride 117.9 mEq/L, calcium
nephrotic syndrome, and cryoglobulinemia.
7.7 mg/dl, uric acid 6.6 mg/dl, albumin 2.9 g/dl. Liver
function tests, prothrombin time, and activated partial
Case Report
thromboplastin time were within normal range.
Electrocardiography revealed normal sinus rhythm,
A 79-year-old woman of Jewish descent was
wide, tall and tended T waves, and S-T segment
admitted with complaints of weakness, leg edema,
depression in leads V1-V2. Urinanlysis
(strip) was
nausea, and weight loss of about 4 kg during the last
protein-positive, with a large number of erythrocytes
month, without fever. Past history was negative for renal
and few leukocytes. Urine osmolarity was 381 mOsm/
disease. Physical examination revealed an ill-looking a
kg, sodium
84.5 mEq/L, potassium
22.3 mEq/L,
febrile patient with pulse
92 bpm, blood pressure
chloride 78 mEq/L; 24-hour urine protein was 6.800
158/72 mmHg
(mild hypertension), and bilateral
mg.
pitting ankle edema (+3) extending proximally to the
Owing to progressive abdominal enlargement and
mid-leg. ere was no organomegaly, although mild to
patient complaints of severe left lower quadrant
moderate ascites was detected. Findings on
abdominal pain, the patient was referred for computed
cardiovascular,
respiratory,
and
neurological
tomography
(without contrast medium). A large
examinations were unremarkable. Chest x-ray did not
peritoneal e usion into the abdomen and pelvis was
show any gross pathology (Fig. 1).
noted, with lymph node enlargement (up to 3.5 cm)
On complete blood work-up, hemoglobin measured
into the pelvis and retroperitoneal and bilateral inguinal
7.3 g/dl (12 g/dl 5 months before), and white blood
lymphadenopathy (Fig. 2).
On subsequent abdominal puncture, done under
local anesthesia, the peritoneal uid was found to be
milky. Laboratory evaluation yielded triglycerides 126
mg/dl, cholesterol 17mg/dl, albumin 0.3 g/dl, glucose
129 mg/dl, lactate dehydrogenase
(LDH) 71 U/L,
establishing the diagnosis of chyloperitoneum. No
evidence of tumor cells was found on cytological
investigation.
Gynecological evaluation did not reveal evidence of
malignancy or other pathology. Skeletal survey was not
suggestive of myeloma. Further laboratory work-up
yielded the following ndings: hepatitis C Ab
-
Figure 1. Chest x-ray did not show any gross
pathology on admission
nonreactive, hepatitis Bs Ag - nonreactive, occult blood
A
B
C
Figure 2. Abdominal CT scan showing large peritoneal e usion and lymph node enlargement in the peritoneal cavity,
pelvis, and retroperitoneal and bilateral inguinal spaces
50
Solun et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
in stool - positive, complement C3 - 58.2 mg/dl (normal
Combined treatment was started with rituximab
range 86-184 mg/dl), complement C4 - 11.2 mg/dl
(Rituxan®, Genentech, Inc., San Francisco, CA) 375
(normal range 20-59 mg/dl), kappa free light chains
mg/m2 every
3 weeks, dexamethasone
(DexPak®,
20.2 mg/dl (normal range 0.14-2.42 mg/dl), lambda free
Mikart, Inc., Atlanta, GA)
40 mg once daily, and
light chains 6.98mg/dl (normal range 0.02-0.67 mg/dl),
chlorambucil
(Leukeran®, GlaxoSmithKline LLC,
immunoglobulin G (IgG) 433 mg% (normal range 600-
Philadelphia, PA) 2 mg once in 2 days. Creatinine level
1600 mg%), immunoglobulin A 64.6 mg% (normal
gradually decreased to 1.5 mg/dl, and urinary protein,
range 100-430 mg%), immunoglobulin M 22.2 mg%
to
229 mg. Nevertheless, the leg edema and ascites
(normal range 40-200 mg%). Serum cryoglobulin assay
remained largely unchanged.
was positive. Bone marrow biopsy demonstrated di use
After 4 courses of therapy, fever developed with
spread of a large number of small lymphocytes,
progressive dyspnea.
e patient was admitted to
compatible with the diagnosis of CLL (Fig. 3).
another hospital with severe right pneumonia
Renal biopsy showed a pattern of MPGN, with a
complicated by lung abscess and pleural empyema.
single thrombus and focal exudative lesions. Direct
Despite drainage of the empyema cavity and intensive
immuno uorescence stain revealed the presence of IgG.
antibiotic therapy, the patient’s status continued to
On electron microscopy, sub endothelial deposits with a
deteriorate, and she died of respiratory and heart failure
micro tubular pattern measuring about 30 nanometers
4 months after the treatment onset.
were noted, compatible with cryoglobulin (Fig. 4).
A
B
CD20-positive B cells (× 20)
CD5-positive B cells on membranous staining
(× 20)
C
D
CD3-positive proliferating T-cells (× 20)
Small lymphocyte cell in ltration of the bone
marrow (HE staining × 20)
Figure 3. Bone marrow biopsy ndings. (A) CD20-positive B cells (× 20). (B) CD5-positive B
cells on membranous staining (× 20). (C) CD3-positive proliferating T-cells (× 20). (D) Small
lymphocyte cell in ltration of the bone marrow (HE staining × 20)
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
51
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
A
B
Fibrinoid necrosis present in a small arteriole
Glomerulonephritis with
(× 100)
membranoproliferative-like pattern showing
a single thrombus and focal exudative lesions
(× 100 )
C
D
Direct immuno uorescence stain of IgG
Electron microscopy picture showing sub
(× 200)
endothelial deposits with micro tubular
pattern measuring about 30 nanometer,
compatible with cryoglobulin
Figure 4. Renal biopsy. (A) Fibrinoid necrosis present in a small arteriole (× 100 magni cation);
(B) Glomerulonephritis with membranoproliferative-like pattern showing a single thrombus and
focal exudative lesions (× 100 magni cation); (C) Direct immuno uorescence stain of IgG
(× 200 magni cation); (D) Electron microscopy picture showing sub endothelial deposits with
micro tubular pattern measuring about 30 nanometer, compatible with cryoglobulin
Discussion
accompany CLL [1]. e others include crescentic
glomerulonephritis, light-chain deposition disease,
CLL is the most common type of leukemia in the
amyloidosis, and focal segmental glomerulosclerosis.
elderly in Western countries and accounts for 30% of all
MPGN may be caused by cryoglobulinemia,
leukemia’s in the United States [7]. Kidney injury in
predominantly type I, eventually associated with
patients with CLL is usually associated with direct
organized sub endothelial or mesangial deposits and
leukemic in ltration and is a common occurrence.
protein thrombi with micro tubular organization. Cryo
However, glomerular involvement leading to proteinuria
crystal globulinemia is characterized by highly organized
of varying severity and nephrotic syndrome is
crystalline substructures a ecting various organs,
exceptionally rare. It is usually a consequence of di use
especially the kidneys and synovial [9,10].
in ltration of the renal tubules and compression of the
Cryoglobulinemia is characterized by the presence of
microvasculature, resulting in intrarenal obstruction
abnormal proteins
(mostly immunoglobulin) in the
and ischemia [2,8]. MPGN is the most common of the
blood that become solid and precipitate at reduced body
di erent types of glomerular pathologies that may
temperatures. In 1933, Wintrobe and Buell [11] were
52
Solun et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
rst to describe “cold precipitable serum globulin” in a
Escherichia coli, and Klebsiella pneumoniae account for
patient with signs and symptoms of hyper viscosity
bacteremia and septicemia in patients with chemotherapy-
associated with multiple myeloma.
e term was
induced neutropenia associated with sustained and
changed to cryoglobulin by Lerner and Watson [12] in
profound T-cell immunode ciency [24,25].
e cellular
1947. According to the classic Brouet classi cation,
immune suppression may also lead to infection by
cryoglobulinemia may be divided into three groups by
opportunistic pathogens, such as Pneumocystis, Listeria,
the type of antibody produced [13]. Type I (simple
Nocardia, Mycobacterium, herpes viruses, and Candida
cryoglobulinemia) is the result of mostly a single
and Aspergillus [26,27]. e respiratory tract is the most
monoclonal IgM, although IgG, IgA, and
common site of infection (advanced severe pneumonia),
immunoglobulin light chains have been reported [14]. It
followed by the urinary tract, skin, and soft tissues. In a
is usually associated with lymphoproliferative disorders,
retrospective study of 402 patients with CLL treated
such as multiple myeloma, CLL, and Waldenstrom’s
with udarabine alone or in combination with
macroglobulinemia. Type II contains monoclonal
corticosteroids, Anaissie et al. [28] noted a 58% rate of
rheumatoid factor, usually IgM, and a polyclonal
major infections in the previously treated patients
component. Type III contains polyclonal IgG and IgM
compared to 34% in the previously untreated patients.
components. Types II and III are also referred to as
On multivariate analysis, signi cant and independent
mixed cryoglobulinemia and account for 80% of all
risk factors for infection were advanced stage of disease
cases of cryoglobulinemia. ey are more often found in
(Rai III and IV), history of previous chemotherapy (or
patients with chronic infections and autoimmune
poor response), elevated serum creatinine level, low
disease. Most patients with mixed cryoglobulinemia
serum albumin level, and low granulocyte count.
have chronic hepatitis C infection [15,16,17].
Type I cryoglobulinemia is characterized by lesions
Conclusion
in nondependent areas
(head and mucosa) and
manifested in the form of Raynaud phenomen, livedo
is report describes a patient with CLL
reticularis, and ulcerations
[18,19]. Musculoskeletal
complicated by acute renal failure, nephrotic syndrome,
manifestations occur in 35%-72% of cases, more often
and cryoglobulinemia. Although renal involvement due
in types II and III. Renal diseases, reported in 5% to
to direct leukemic in ltration is relatively common in
60% of patients with cryoglobulinemia, and neuropathy,
patients with CLL, acute renal failure with nephrotic
reported in 10% to 80%, are also usually associated
syndrome and cryoglobulinemia is extremely rare.
with the mixed types. Less frequent manifestations
MPGN is the most common glomerular pathology in
include abdominal pain (2%-22%), acrocyanosis (9%),
patients with CLL. Treatment with chlorambucil,
and arterial thrombosis (1%). Renal involvement is one
prednisolone, and monoclonal antibodies stabilizes the
of the most serious complications of cryoglobulinemia.
renal function. Infection is a major risk factor in the
It usually appears within 3-5 years of the diagnosis, with
clinical course of CLL and a leading cause of morbidity
a higher prevalence in mixed cryoglobulinemia
and mortality.
e pathogenesis of infection in this
[17,20,21]. Clinically, the most common features of
setting is multifactorial and usually associated with
renal involvement are isolated proteinuria and
hypogammaglobulinemia and treatment with
hematuria, either microscopic or macroscopic, followed
immunosuppressant’s and monoclonal antibodies. In
by nephritic/nephrotic syndrome and acute renal failure
our patient, renal function improved after treatment
[22].
rituximab, dexamethasone, and chlorambucil, but she
Patients with CLL are prone to infectious
died several months later from severe complications of
complications, which are the leading cause of CLL-
pneumonia.
related morbidity and mortality; studies show that
infections are responsible for 30% to 50% of all deaths
[23]. Susceptibility to infections is associated with
References
hypogammaglobulinemia
and
further
immunosuppression secondary to the treatment with
1. Favr Favre G, Courtellemont C, Callard P, et al.
steroids,
immunosuppressants, and monoclonal
Membranoproliferative glomerulonephritis, chronic
antibodies. Most of the infections are bacterial in origin;
lymphocytic leukemia, and cryoglobulinemia. Am J
the main culprits are encapsulated bacteria such as
Kidney Dis 2010;55(2):391-4.
Streptococcus pneumoniae and Haemophilus in uenzae.
2. Dou X, Hu H, Ju Y, et al. Concurrent nephrotic
Gram-negative pathogens such as Pseudomonas aeruginosa,
syndrome and acute renal failure caused by chronic
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
53
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
lymphocytic leukemia (CLL): a case report and literature
cryoglobulinaemia, and vasculitis: immune complex
review. Diagn Pathol 2011;6:99. Doi: 10.1186/1746-
relations. Lancet Infect Dis 2005;5:227.
1596-6-99.
17.
Sene D, Ghillani-Dalbin P, ibault V, et al. Long-
3.
Mutluay R, Aki SZ, Erten Y, et al. Membranoproliferative
term course of mixed cryoglobulinemia in patients
glomerulonephritis and light-chain nephropathy in
infected with hepatitis C virus. J Rheumatol
association with chronic lymphocytic leukemia. Clin
2004;31:2199-206.
Nephrol 2008;70(6):527-31.
18.
Monti G, Galli M, Invernizzi F, et al.
4.
Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann
Cryoglobulinaemias: a multi-centre study of the early
M. Biologic and clinical signi cance of cryoglobulins. A
clinical and laboratory manifestations of primary and
report of 86 cases. Am J Med 1974;57(5):775-88.
secondary disease. GISC. Italian Group for the Study
5.
Aslam N, Nseir NI, Viverett JF, Bastacky SI, Johnson
of Cryoglobulinaemias. QJM 1995;88(2):115-26.
JP. Nephrotic syndrome in chronic lymphocytic leukemia:
19.
Rossi D, Mansouri M, Baldovino S, et al. Nail fold
a
paraneoplastic
syndrome?
Clin
Nephrol
videocapillaroscopy in mixed cryoglobulinaemia.
2000;54(6):492-7.
Nephrol Dial Transplant 2004;19(9):2245-9.
6.
Moulin B, Ronco PM, Mougenot B, Francois A,
20.
Ferri C, La Civita L, Cira si C, et al. Peripheral
Fillastre JP, Mignon F. Glomerulonephritis in chronic
neuropathy in mixed cryoglobulinemia: clinical and
lymphocytic leukemia and related B-cell lymphomas.
electrophysiologic
investigations.
J
Rheumatol
Kidney Int 1992;42(1):127-35.
1992;19(6):889-95.
7.
Siegel R, Naishadham D, Jemal A. Cancer statistics,
21.
Satish S, Rajesh R, George K, Elango EM, Unni VN.
2012. CA Cancer J Clin 2012;62(1):10.
Membranoproliferative glomerulonephritis with essential
8.
Rifkin SI. Acute renal failure secondary to chronic
cryoglobulinemia. Indian J Nephrol 2008;18(2):80-2.
lymphocytic leukemia: a casereport. Medscape J Med
22.
Alchi
B,
Jayne
D. Membranoproliferative
2008;10(3):67.
glomerulonephritis. Pediatr Nephrol 2010;25(8):1409-
9.
Galea HR, Bridoux F, Aldigier JC, et al. Molecular
18.
study of an IgG1kappa Cryoglobulin yielding organized
23.
Francis S, Karanth M, Pratt G, et al. e e ect of
microtubular deposits and glomerulonephritis in the
immunoglobulin VH gene mutation status and other
course of chronic lymphocytic leukaemia. Clin Exp
prognostic factors on the incidence of major infections in
Immunol 2002;129(1):113-8.
patients with chronic lymphocytic leukemia. Cancer
10.
PapoT, Musset L, BardinT, et al. Cryocrystalglobulinaemia
2006;107(5):1023-33.
as a cause of systemic vasculopathy and widespread erosive
24.
Morrison VA. Infectious complications in patients with
arthropathy. Arthritis Rheum 1996;39:335-40.
chronic lymphocytic leukemia: pathogenesis, spectrum of
11.
Wintrobe MM, Buell MV. Hyperproteinemia
infection, and approaches to prophylaxis. Clin
associated with multiple myeloma: with report of a case
Lymphoma Myeloma 2009;9(5):365-70.
in which an extraordinary hyperproteinemia was
25.
Nosari A. Infectious Complications in Chronic
associated with thrombosis of the retinal veins and
Lymphocytic Leukemia. Mediterr J Hematol Infect Dis
symptoms suggesting Reynaud’s disease. Bull Johns
2012;4(1):e2012070. Epub
2012 Nov
5. doi:
Hopkins Hosp 1933;52:156.
10.4084/MJHID.2012.070.
12.
Lerner AB, Watson CJ. Studies of cryoglobulins;
26.
Byrd JC, Hargis JB, Kester KE, Hospenthal DR,
unusual purpura associated with the presence of a high
Knutson SW, Diehl LF. Opportunistic pulmonary
concentration of cryoglobulin (cold precipitable serum
infections with udarabine in previously treated patients
globulin). Am J Med Sci 1947;214(4):410.
with low-grade lymphoid malignancies: A role for
13.
Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann
Pneumocystis carinii pneumonia prophylaxis. Am J
M. Biologic and clinical signi cance of cryoglobulins: a
Hematol 1995;49(2):135-42.
report of 86 cases. Am J Med 1974;57:775.
27.
Morrison VA. Infectious complications of chronic
14.
Morra E. Cryoglobulinemia. Hematology Am Soc
lymphocytic leukaemia: pathogenesis, spectrum of
Hematol Educ Program 2005:368-72.
infection, preventive approaches. Best Pract Res Clin
15.
Cacoub P, Costedoat-Chalumeau N, Lidove O, Alric
Haematol 2010;23(1):145-53.
L. Cryoglobulinemia vasculitis. Curr Opin Rheumatol
28.
Anaissie EJ, Kontoyiannis DP, O’Brien S, et al. Infections
2002;14(1):29-35.
in patients with chronic lymphocytic leukemia treated with
16.
Sansonno D, Dammacco F. Hepatitis C virus,
udarabine. Ann Intern Med 1998;129(7):559-66.
54
Solun et al
CASE PRESENTATION
BLADDER LITHIASIS SECONDARY TO A MIGRATED INTRAUTERINE
DEVICE. CASE REPORT
Victor Ona1, Bogdan Feciche2, Andrei Boc1, Dan Ona3, Ioan Coman1
1Clinic of Urology, Municipal Clinical Hospital of Cluj-Napoca, 2Emergency County Hospital of Satu Mare and
3Obstetrics and Gynecology Clinic I of Cluj-Napoca
Address for correspondence:
Ona Victor MD PhD FEBU
Email: ona_victor@yahoo.de
Received: 19.12.2013
Accepted: 23.02.2014
Med Con March 2014, Vol 9, No 1, 55-58
Abstract
is paper presents the case of a 64-year old patient
with this pathology, and we emphasize both the
Although used as e ective methods of contraception
diagnostic aspects and other minimal invasive surgical
for over
30 years, intrauterine contraceptive devices
solutions.
(IUCD) are not free of complications. One of the
known complications of ICUD is migration.
Case report
In this paper, we present the case of a patient of 64
years old with the diagnosis of bladder lithiasis secondary
At the Department of Urology of the Municipal
to the migration of an intrauterine device implanted 20
Clinical Hospital of Cluj-Napoca, at the outpatient care
years earlier. We present the methods that led to the
unit, a 64-year old patient complained of intermittent
above mentioned diagnosis and the minimally invasive
hematuria, unregulated pelvic pain, pollakiuria and
solution for this complication.
dysuria, being referred by another medical service with
Keywords: intrauterine contraceptive devices,
the clinical and ultrasound suspicion of calci ed bladder
bladder lithiasis, endoscopic surgery
tumor. To determine the diagnosis, the patient was
evaluated clinically and para clinically. Her personal
Introduction
medical history showed a caesarian section at the age of
38 and natural menopause that began early, at the age of
Intrauterine contraceptive devices (IUCD) are used
44.
e urine showed microscopic hematuria 12 Ery/µl,
for over 30 years [1]. Although they are known to be
mild leukocyturia 20 Leu/µl with negative nitrites. e
e ective and safe methods of contraception, sometimes
abdominal ultrasound described an atrophic uterus and
these devices present some complications, sometimes
showed a hyperechogen tumor at the level of the bladder
with a signi cant impact on the patient, such as uterine
dome which suggested a suspended bladder calculus.
perforation, pelvic abscess or septic shock. e incidence
Next to the calculus, there was a hyperechogen structure
of uterine perforation caused by IUCD is low. However,
in T-shape with normal uterine cavity in relation to a
the literature mentions about 100 cases of extrauterine
menopausal age of 20 years. A simple abdominal X-ray
migration of these devices [2].
plain lm presented a radio- opaque image at projection
Late intrabladder migration of intrauterine devices
area in the urinary bladder, suggestive for lithiasis that
(IUD) represents a very rare event, which may be the
had attached an intrauterine device in abnormal
source of bladder calculi.
anatomic position - presented in Figure 1.
Bladder Lithiasis Secondary to a Migrated Intrauterine Device. Case Report
55
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
A
B
Figure 1. Pelvis X-ray image presents a calcareous tumor at projection in the urinary bladder,
attached to an intrauterine device in non-anatomic position (A), intrauterine device, detail (B)
Figure 2. Endoscopic aspect of the lithiasis
developed on the migrated intrauterine device
in the bladder
Figure 3. Lithotripsy with LASER Holmium through the device inserted on the work canal
of the cytoscope
e anamnesis was performed again, and the patient
and then we made the linear incision of the bladder
mentioned that at the beginning of the ’90s an IUD was
mucous membrane above the IUD (Figure 3).
inserted and she has not made any gynecological
Extraction of the IUD, by means of an extracting
examination since then. We performed cystoscopic
endoscopic clip, Figure 4.
e mucous membrane has
examination and we determined the diagnosis of bladder
minimum spotting. At the end of the intervention, a
lithiasis developed on top of a migrated intrauterine
bladder Foley 16 Ch catheter was inserted.
device, partially incorporated into urinary bladder wall. In
Postoperative recovery was favorable, with discharge
Figure 2 we may see the cytoscopic aspect of the bladder.
after 48h, and the urinary catheter was taken out after
Endoscopic lithotripsy of bladder with Holmium
14 days. e follow-up examination 3 months after the
LASER device was indicated and performed under
surgery revealed an optimal status from bacteriological,
spinal anesthesia.
e lithotripsy was performed rst, ultrasound and cytoscopic points of view. (Figure 5)
56
Ona et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
Figure 4. IUD extracted endoscopically
Figure 5. e endoscopic aspect of the bladder
wall at the follow-up cystoscopy, 3 months
after surgery shows optimal healing
Discussions
Most of the authors recommend taking out the
intrauterine devices that contain copper, because of the
is case is particular by its exception, the long
possibility of in ammatory reaction that may cause
period of IUD insertion, diagnosis and treatment.
occlusion or intestinal perforation. Besides, there are
In the case presented above there was an interval free
reasons for removing all migrated intrauterine devices.
of symptoms between the device insertion and the
ese include the functional compromise of the adjacent
occurrence of the urinary manifestations that involved
structures, infection and anxiety of the patient after the
paraclinical explorations that showed the migrated foreign
determination of the diagnosis of foreign body in the
body in the bladder, which was subject to mineral coating
abdomen [4].
that led to the confusion of calci ed bladder tumor. We
Although laparoscopy is preferred to classic surgical
believe that the short experience with IUD at the moment
exploration, we still have to take into consideration the
of insertion was an important factor for late complications.
possibility of conversion because of the di culties
e role of minimally invasive endoscopic surgery is
encountered in the case of these interventions [3].
essential and the favorable evolution is a consequence of
Between
1999-2009, the literature mentioned
the surgical technique that complies with the continuity
another
9 cases of bladder lithiasis secondary to a
of urothelium.
migrated intrauterine device [1,2,5-10].
e intra-abdominal migration of an intrauterine
It is considered that the occurrence of a continuity
contraceptive device is very rare. A review of the
area at the level of the uterus takes place or starts on the
literature, extended for 18 years published in 1999 by
insertion, as there is the risk in 2.2 cases out of 1000
Kassak and Audra [3], reported 165 cases of intra-
insertions
[11].
e correct insertion of an IUD
abdominal migration of IUCD. ese were localized in
involves the compliance with indications and
the omentum in 23 cases, recto sigmoid in 44 cases,
contraindications, of which some are absolute, others
peritoneum in 41 cases, bladder in 23 cases, appendix in
are relative.
e presence of uterine scar after Caesarian
8 cases, small intestine in 2 cases, annex in 1 case and
section increases the risk of complete or partial
respectively iliac vein 1 in case.
perforation of the uterus where the resistance is lower.
Bladder Lithiasis Secondary to a Migrated Intrauterine Device. Case Report
57
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Usually, the perforation of the uterus because of local
4.
Ozgun MT, Batukan C, Serin IS, Ozcelik B, Basbug
anatomic conditions occurs in the fundic zone.
e
M, Dolanbay M. Surgical management of intra-
failure to recognize immediately this accident may be
abdominal
mislocated
intrauterine
devices.
solved by celioscopy. In some cases, the presence of
Contraception 2007;75(2):96-100.
anatomical neighborhood relations with the bladder-
5.
Insausti Jaca N, Urresola Olabarrieta A, Ibáñez S, et
uterine peritoneal fold, distended, and the presence of
al. Uterovesical perforation secondary to intrauterine
an altered area of myometrum caused by segment
device with vesical lithiasis formation: a report of two
incision of a Cesarean section are a local irritating cause
cases. Radiologia 2007;49(2):129-32.
manifested by menometrorrhagia or the possibility of
6.
Singh I. Intravesical Cu-T emigration: an atypical and
complete or partial migration of the IUD into the
infrequent cause of vesical calculus. Int Urol Nephrol
bladder.
2007;39(2):457-9.
In conclusion, bladder lithiasis which develops
7.
Hick EJ, Hernández J, Yordán R, Morey AF, Avilés R,
intravesically on top of a migrated IUD is a rare clinical
García CR. Bladder calculus resulting from the
situation, but not impossible to see in practice.
e
migration of an intrauterine contraceptive device. J Urol
minimally invasive endoscopic surgery using the
2004;172(5 Pt 1):1903.
instruments of the endoscopic surgery is possible, and
8.
Iturralde Codina A, Gozá León F, Beyríes Tamayo W,
the evolution after surgery is optimal.
Iturralde Muñoz Y, Rodríguez Hidalgo ME. Double
bladder lithiasis from an intrauterine device. Report one
case. Arch Esp Urol 2004;57(2):160-2.
Bibliography
9.
Ozçelik B, Serin IS, Basbug M, Aygen E, Ekmekçioglu
O. Di erential diagnosis of intra-uterine device
1. Mustafa M. Erosion of an intrauterine contraceptive
migrating to bladder using radiographic image of
device through the bladder wall causing calculus:
calculus formation and review of literature. Eur J Obstet
management and review of the literature. Urol Int
Gynecol Reprod Biol 2003;108(1):94-6.
2009;82(3):370-1.
10.
Nouri M, Fassi M, Koutani A, Ibn Attya A, Hachimi
2. Ozgür A, Sişmanoğlu A, Yazici C, Coşar E, Tezen D,
M, Lakrissa A. Migration of an intrauterine device into
Ilker Y. Intravesical stone formation on intrauterine
the bladder. Report of a case. J Gynecol Obstet Biol
contraceptive device. Int Urol Nephrol 2004;36(3):345-
Reprod (Paris) 1999;28(2):162-4.
8.
11.
E. Caliskan, N. Ozturk, B.O. Dilbaz, S. Dilbaz.
3. Kassab B, Audra P. e migrating intrauterine device.
Analysis of risk factors associated with uterine perforation
Case report and review of the literature. Contracept
by intrauterine devices. Eur J Contracept Reprod
Fertil Sex 1999;27(10):696-700.
Health Care 2003;8(3):150-5.
58
Ona et al
MEDICINE AND ART
PAINTINGS OF A CASE OF OBESITY IN THE 17TH CENTURY, PROBABLY
DUE TO PRADER WILLI SYNDROME
Călin Bumbulu1, Andrei Bumbulu2, Alina Daniela Negru1, Rumelia Koren3
1SCM dr Bumbulu - dr Balaj, Satu Mare, România, 2Faculty of Medicine, Iuliu Ha ieganu University of Medicine and
Pharmacy, Cluj Napoca, România, 3Department of Pathology, Hasharon Hospital, Petah Tikva, and Sackler Faculty of
Medicine, Tel-Aviv University, Israel
Address for correspondence:
Bumbulu Călin, MD, FP
Satu Mare, str. Bobocului UK 30-440258
Email: bumbulutcalin@yahoo.com
Received: 06.10.2013
Accepted: 10.12.2013
Med Con March 2014, Vol 9, No 1, 59-62
Abstract
depicting 3615 inhabitants of a de ned geographical
region and covering several centuries, overweight in
During the Middle Ages and the Renaissance
people was more common in men than in women (30%
obesity was often seen as a sign of wealth. In our days we
vs. 44%). Overweight was most common in sitters aged
know that obesity are bad for health, and obesity
>40 than in those aged 40 or younger. Other conditions,
prevention is a public health imperative. We present two
such as amputated limbs, missing teeth, or osteoarthritis
portraits of Eugenia Martínez Vallejo, an 8 year old girl
deformations were surprisingly rare in the portraits
who was called “ e Monster” due to her obesity caused
under evaluation.
e association between overweight
probably by Prader-Willi Syndrome, painted by one of
and higher age was most pronounced during the 17th
the most highly esteemed court painters of 17th century,
and 18th centuries. During the 18th century among
Juan Carreño de Miranda.
people over 40, 79% of men were overweight compared
Keywords: Prader-Willi Syndrome, obesity,
with 51% of women. From the 18th to the 20th century
painting, Juan Carreño de Miranda
the prevalence of overweight decreased in men over 40.
In Figure 1 is an example of the Baroque taste for
e image we each have of our own body,
representations of freaks of nature and the attraction of
profoundly a ects the way how we relate to society.
people with some of physical or psychological anomaly.
Depictions of obesity in art provide a context for
In that painting it takes the form of a depiction of a
thinking about the changing meaning of obesity to
girl of extraordinary size, probably due to Prader-Willi
individuals and society. During the Middle Ages and the
syndrome [3].
e placement of the model over a
Renaissance obesity was often seen as a sign of wealth,
neutral background follows the tradition of Spanish
and was relatively common among the elite [1]. Of
court portraiture. Eugenia Martínez Vallejo was taken
course, in our days we now that obesity are bad for
to the court in 1680 and her portrait was painted there
health, and obesity prevention is a public health
at the order of King Carlos II. She was one of the
imperative.
individuals with physical or psychological defects that
In a systematic review of portraits and description
formed a small court around the Spanish royal
of visible signs of illness [2] on a collection of portraits
children.
Paintings of a Case of Obesity in the 17th Century, Probably Due to Prader-Willi Syndrome
59
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Figure 1. Juan Carreño de Miranda, “Eugenia Martínez Vallejo, La monstrua vestida”, oil on canvas,
Madrid, Museo del Prado
Figure 2. Sculpture of Eugenia Martínez Vallejo
by Amado González Hevia, Aviles, Spain
60
Bumbuluț et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
MEDICINE AND ART
e 8 year old girl was called “ e Monster” due to
It is said that upon seeing the painting in the Prado
her obesity. Another painting exists with Eugenia
Museum, Dr. Andrea Prader immediately recognized
without clothes. Both paintings are in the Prado
her features to be consistent with Prader-Willi
Museum. Her deformity is emphasized by the beautiful
Syndrome. Although we may never know if this child
owered red dress that drapes over the huge size of her
did in fact have PWS, the painting and descriptions of
body. Its color makes the nudity of the companion
her condition strongly support this hypothesis.
is
painting all the more explicit.
painting is regarded as the earliest illustrations of PWS.
Eugenia Martínez Vallejo was paraded around on
La Monstrua has continued to be an intriguing gure as
fairs to crowds.
e role played by these individuals at
evidenced by an outdoor sculpture in Aviles created in
the Court was often important. ey provided company
1997 by the Spanish artist Amado González Hevia who
for the princes and princesses and because their height
based his sculpture on Juan Carreño de Miranda’s
was similar to that of the children the Infantes felt at
portraits of Eugenia (Figure 2).
ease with them. eir age meant the royal children had
e maternal origin of the genetic material that is
a permanent con dante who assured that they were
a ected in the syndrome is important because the region
always taken care of as well as providing them with
of chromosome 15 involved, one of the most complex
entertainment. When they were older, the princes and
regions of the human genome, is subject to parent of
princesses often kept these childhood friends at their
origin imprinting, meaning that for a number of genes
sides such as Philip II’s daughter, Isabel Clara, who was
in this region only one copy of the gene is expressed
often portrayed along with her own dwarf and cried
while the other is silenced through imprinting. For the
more than anyone when she died.
genes a ected in PWS, it is the maternal copy that is
is portraits was painted by one of the most highly
usually imprinted
(and thus is silenced), while the
esteemed court painters, Juan Carreño de Miranda (25
mutated paternal copy is not functional.
is means
March 1614-3 October 1685), who used Eugenia as a
that while most people have a single working copy of
model on a number of occasions. Juan Carreño depicted
these genes, people with PWS have a non-working copy
life at the court of Charles II better than any other
and a silenced copy. If the maternally derived genetic
painter, revealing the weakness of the king who came to
material from the same region is a ected instead, the
be known as “the Bewitched”. He refused to be knighted
result is the oposite syndrome - Angelman syndrome.
in the order of Santiago, saying
“painting needs no
Nowdays, with the recent bene ts of early diagnosis
honors, it can give them to the whole world”. Noble by
and ongoing interventions, the obesity rate among
descent, he had an understanding of the workings and
children with Prader-Willi Syndrome has decreased to
psychology of the royal court as no other before him,
be similar to the typical population.
making his portraits of the Spanish royal family in an
Angelman, Prader-Willi, and Chromosome
15q
unprecedented documentary fashion. Most of his works
Duplication syndromes are speci c conditions caused
are portraits of the royal family and court, though there
by di erent genetic variants in the same genetic region.
are early works commissioned mainly by the church,
November 15th was declared e International 15q Day,
some altarpieces.
to raise awareness of the similarities between the
Prader-Willi syndrome
(PWS) is a rare, genetic
syndromes.
disorder in which seven genes on chromosome 15 are
deleted or unexpressed
(chromosome
15q partial
deletion) on the paternal chromosome. e syndrome
References
was rst described in 1956 by Andrea Prader, Heinrich
Willi, Alexis Labhart, Andrew Ziegler, and Guido
1. Ferrucci L, Studenski SA, Alley DE, Barbagallo M,
Fanconi. Characteristic of PWS is small hands and feet,
Harris TB. Obesity in Aging and Art. J Gerontol A
short stature, low muscle tone, incomplete sexual
Biol Sci Med Sci 2010;65A(1):53-56.
development, cognitive disabilities, problem behaviors,
2. Als C, Stüssi Y, Boschung U, Tröhler U, Wäber JH.
and a chronic feeling of hunger that can lead to excessive
Visible signs of illness from the 14th to the 20th century:
eating and life-threatening obesity.
e incidence of
systematic review of portraits. BMJ 2002;325(7378):1499.
PWS is between 1 in 25,000 and 1 in 10,000 live births.
3. Pozzilli P, Khazrai YM. “La Monstrua Vestida”, a case
PWS a ects males and females with equal frequency
of Prader-Willi syndrome. J Endocrinol Invest
and a ects all races and ethnicities.
2005;28(2):199.
Paintings of a Case of Obesity in the 17th Century, Probably Due to Prader-Willi Syndrome
61
Corso, Center of Satu Mare City
(Corso, Centrul oraşului Satu Mare)
Roman-Catholic Cathedral, Freedom Square
(Catedrala romano-catolică, Pia a Libertă ii)
GUIDANCE FOR DRAWING UP
GUIDANCE FOR AUTHORS
Scope
on which patients or other subjects of your experiments
e Medical Connections publishes papers reporting
clearly grant permission for the publication of
original clinical and scienti c research, which contribute
photographs or other material that might identify them.
to the advancement of knowledge in all eld of medicine.
If the consent form for your research does not speci cally
e journal also publishes reviews, editorials and short
include this, please obtain it or remove the identifying
communications on speci c topics. Case reports will be
material. A statement must be included in the ‘Methods’
accepted if of great interest and well investigated. Letters
section of your paper.
to the Editor, especially those mentioning an opinion on
an article previously published, or expressing a new
Ethics Committee approval
nding are welcome. e website address of the Medical
You must state clearly in your submission in the
e
Methods section that you conducted studies on human
journal is published quarterly and papers are accepted
participants with the approval of the Hospital, or
for publication in English language. Papers from
University Ethics Committee etc. Similarly, you must
contributors living abroad and from Romanian authors
con rm that experiments involving animals adhered to
should be addressed to the editorial o ce: dr. Bumbulu
ethical standards.
Călin, assitant editor in chief of Medical Connections,
Eroilor Revolu iei Pl. no.23-440055 Satu Mare,
Copyright assignment
Romania. Tel./Fax:
+40-261-710456,
e-mail:
Papers are accepted for publication on the
bumbulutcalin@yahoo.com.
understanding that exclusive copyright in the paper is
assigned to the Publisher. Authors may use material
Redundant or duplicate publication
from their paper in other works published by themselves.
We ask you to con rm that your paper has not been
published in its current form or a substantially similar
Submissions
form, that it has not been accepted for publication by
All manuscripts submitted to the Medical
another journal, and that it is not under consideration
Connections are made available for online review.
e
by another publication.
journal introduced the electronic submission of
manuscripts in Word format, but also accepts
Conflicts of interest
manuscripts submitted as attachments to electronic
We ask authors to state all possible con icts of
mail (text, gures and tables). Do not send them in
interest, including nancial and other relationships. If
PDF format. e word count for electronic submissions
you are sure that there is no con ict of interest, please
is up to 3,500 words for original articles, 2,500 words
state this also.
e sources of funding should be
for case reports, 2,000 for clinical imaging papers, 500
acknowledged in your paper.
words for letters, and 4,500 words for review articles.
Authors should NOT in addition post a hard copy
Permissions to reproduce previously
submission to the editorial o ce, unless they are
published material
supplying artwork, letters or if les that cannot be
Please send us copies of permission to reproduce
submitted electronically, or have been instructed to do
material (such as illustrations) from the copyright holder.
so by the editorial o ce. For those authors who have no
option but to submit by mail please send one copy of
Patient consent forms
the article, plus an electronic version on CD-ROM to
e protection of a patient’s right to privacy is
the Editorial O ce, Conexiuni Medicale/Medical
essential. Please send copies of patient’s consent forms
Connections, Eroilor Revolu iei Pl. no.23-440055 Satu
63
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Mare, Romania. Double spacing should be used
Review articles and case reports should include an
throughout the manuscript, which should include the
unstructured summary.
following sections, each starting on a separate page: title
Key words
page, abstract and key words, text, acknowledgements,
e abstract should be followed by a list of 3-10
references, individual tables and legend for gures. Pages
keywords or short phrases which will assist the cross-
should be numbered consecutively, beginning with the
indexing of the article and which may be published.
title page, and the Arabic numbers should be placed in
When possible, the terms used should be from the
the top right hand corner of each page.
Medical Subject Headings 262 list of Index Medicus
Presentation of papers
Text
Title page
Full papers of an original study may be divided into
e title page should carry the full title of the paper
sections headed Introduction, Methods (including ethical
and a short title to be used as a short ‘running head’ (and
and statistical information), Results and Discussion
which should be so identi ed and should comprise up to
(including a conclusion).
is so-called
“IMRAD”
45 characters).
e rst name, middle initial and last
structure is not simply an arbitrary publication format,
name of each author should appear. If the work is to be
but rather a direct re ection of the process of scienti c
attributed to a department or institution, its full name
discovery. Long articles may require subheadings within
should be included. Any disclaimers should appear on the
some sections (especially the Results and Discussion
title page, as should the name and address of the author
sections) to clarify their content. Other types of articles,
responsible for correspondence concerning the manuscript
such as case reports, reviews, and editorials, are likely to
and the name, address and e-mail address of the author to
require other formats. Excessive use of abbreviations is
whom requests for reprints should be made (the author
not recommended. Outline statistical methods used.
should mention if he does not want his e-mail address to
Identify drugs and chemicals used by generic name (if
be published). Finally, the title page should include the
trade-marks are mentioned, manufactured name and
sources of any support for the work in the form of grants,
city should be given).
equipment, drugs, or any combination of these.
Acknowledgements
Abstracts
Acknowledgements should be made only to those
e second page should carry a structured abstract
who have made a substantial contribution to the study.
of no less than 200 words. Do not use abbreviations,
Authors are responsible for obtaining written permission
footnotes, or references.
from people acknowledged by name in case readers infer
Background & Aims
their endorsement of data and conclusions.
Describe the importance of the study and the
References
precise research objective(s) or study question(s).
References should be numbered consecutively in
Methods
the order in which they rst appear in the text.
ey
Methods should include information on the following
should be assigned Arabic numerals, which should be
aspects of study design when applicable: Design - describe
given in brackets, e.g. [12]. References should include
the basic study design, e.g. randomized controlled trial,
the names of all authors when six or fewer; when seven
cross sectional study, cohort study, case series, survey etc;
or more, list only the rst three names and add et al.
Setting - specify whether the study was conducted in a
References should also include full title and source
primary or tertiary care setting, in an ambulatory care
information. Journal names should be abbreviated as in
clinic or hospital, in the general community etc;
Index Medicus
Participants - indicate the number of study subjects and
terms_cond.html). No more than 90-100 references
how they were selected, recruited, and assigned to the
will be accepted for reviews. For Letters to the Editor,
intervention; Intervention
- report the method of
5-6 references. Avoid or keep as low as possible the use
administration and duration of the intervention.
of abstracts as references. Personal communications and
Results
unpublished work should not feature in the reference
Provide the main outcomes of the study, including
list but should appear in parentheses in the text.
con dence intervals or p values.
Unpublished work accepted for publication but not yet
Conclusion
released should be included in the reference list with the
State only conclusions that are directly supported
words “in press” in parentheses beside the name of the
by the evidence and the implications of the ndings.
journal concerned.
64
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
GUIDANCE FOR DRAWING UP
a) Article:
in the metric system in terms of the International
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
System of Units (SI).
MA, Holub MC, Kovalsykz I, et al. Toward understanding
Abbreviations and symbols
the role of leptin and leptin receptor antagonism in
Use only standard abbreviations. Avoid
preclinical models of rheumatoid arthritis. Peptides
abbreviations in the title and abstract.
e full term for
2011;32:1567-74.
which an abbreviation stands should precede its rst use
b) Papers published only with DOI numbers:
in the text unless it is a standard unit of measurement.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Reprints
vascular periadventitial adipose tissue (tunica adiposa) as
Ten reprints of the published articles and two copies
an example. Cell Biol Int
2011;doi:
10.1042/
of the Journal will be supplied free of charge. If required
CBI20110422.
in a greater number, they will be available on payment
c) Book:
of the necessary cost.
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Landes Bioscience, Austin, Texas, USA. 2009.
Editorial policy
d) Book chapter:
We welcome all contributions in the eld of
[4] Jeremy L, Abe PD. Treatment Options in
medicine. We invite known personalities with expertise
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
and many published papers in a speci c eld to write
cancers in clinical practice, Springer-Verlag, London
reviews and editorials in our journal. We accept original
Limited, 2007:75-102.
papers and case reports from all countries.
e
Tables
Conexiuni Medicale/Medical Connections o ers
Each table should be assigned a Roman numeral
thorough peer review and immediate publication on
(e.g. Table III) and a brief title. Explanatory matter
acceptance.
e redactor-in-chief or one of the rst
should be placed in footnotes. Explain in footnotes all
reads the manuscripts received and in about 1-3 weeks
non-standard abbreviations that are used in each table.
decide upon their priority level: some are immediately
Identify statistical measures of variations, such as
sent to the reviewers, some are rejected without being
standard deviation and standard error of the mean. Each
sent for review and some are returned to authors with
table should be cited in the text.
suggestions for improvement before submitting them
Illustrations
to reviewers.
All graphs, photographs (on glossy paper), diagrams
will be referred to as gures and should be numbered
Peer-review procedure
consecutively in the text in Arabic numerals. If a gure
e Conexiuni Medicale/Medical Connections
has been published before, the original source must be
promotes evaluation of all the original papers by two or
acknowledged and written permission from the
three independent reviewers, of whom two are
copyright holder for both print and electronic formats
international personalities.
e peer-review process is
should be submitted with the material. Figures may be
essential for ensuring the quality of the scienti c
reduced, cropped or deleted at the discretion of the
information disseminated.
e reviewers are asked to
Editor.
evaluate the manuscript by applying the same standards
Legends for illustrations
as for the international journals.
e reviewers send
Captions should have an Arabic numeral
their comments to the Editor. e Editor will inform
corresponding to the illustration to which it refers with
the authors about the suggestions made by the referee
a title above and explanatory notes below it. Internal
and ask them to answer the questions and make the
scales should be explained and staining methods for
required corrections. is information is provided up to
photomicrographs should be identi ed.
three months from the date they submitted the paper to
Units of measurement
the journal. e revised manuscript should be sent in no
Measurements of length, height, weight, and
more than one month to the Editor. When the Editor
volume should be reported in metric units
(meter,
receives the corrected version with all changes marked,
kilogram, or litre) or their decimal multiples.
accompanied by a letter with a point-by-point reply to
Temperatures should be given in degrees Celsius. Blood
the reviewers’ comments, he sends those back to the
pressures should be given in mmHg. All hematological
same reviewer, who makes the nal recommendation for
and clinical chemistry measurements should be reported
acceptance or rejection of the manuscript.
65
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Notice to subscribers
inside front or inside back cover: Euro 350 1 issue, 1400
e annual subscription rates for 2014: 80 RON
4 issues. Full colour page ouside back cover: Euro 400 1
individual, 160 RON institutional. Foreing subscribers:
issue, 1600 4 issues. Bank account: Colegiul Medicilor
75
$ individual, 150
$ institutional. Additional postage:
Satu Mare, CUI 9839430, Banca Transilvania, branch
surface mail 20
$, for overseas air mail 40
$. Bank
Agen ia Golescu Satu Mare, IBAN: RO38 BTRL 0310
account: Colegiul Medicilor Satu Mare, CUI 9839430,
1202 K392 62XX (RON) IBAN: RO62 BTRL 0310
Banca Transilvania, branch Agen ia Golescu Satu Mare,
2202 K392 62XX (USD) Swift: BTRLRO22.
IBAN: RO38 BTRL 0310 1202 K392 62XX (RON)
IBAN: RO62 BTRL 0310 2202 K392 62XX (USD)
© Copyright Conexiuni Medicale/Medical
Swift: BTRLRO22. Orders should be sent to the
Connections, Satu Mare, 2014
Editorial O ce, Eroilor Revolu iei Pl. no.23-440055
No part of this publication may be reproduced,
Satu Mare, Romania. Tel./Fax:
+40-261-710456 or
stored in a retrieval system or transmitted in any form or
+40-361-408164, or by e-mail: colmedsm@gmail.com.
by any means without prior permission in writing of
Conexiuni
Medicale/Medical
Connections.
Notice to advertisers
Permission is not however required to copy abstracts of
Applications for advertisement space and for rates
papers or of articles on condition that a full reference to
should be addressed to the Editorial O ce of Conexiuni
the source is shown. Correspondence regarding
Medicale/Medical Connections.
2014 advertising
permission to reprint all or part of any article
rates are Euro 200 full (A4) colour page, 1 issue, and
published in this journal should be addressed to the
Euro 800 full colour page, 4 issues. Full colour page on
Editor, e-mail: colmedsm@gmail.com
66
EDITORIAL
PUTEREA IDEOLOGIILOR
„- Iubitule, mă mai iubeşti?
- Te voi iubi veşnic, iubita mea!”
Acest dialog aproape banal nu este despre iubire,
vorba doar de „liberalizarea” asigurărilor. Vom avea mai
cum ar părea la prima vedere. Este despre certitudine,
multe case private de asigurări de sănătate, pacien ii vor
certitudinea iubirii în acest caz. Oamenii sunt amânzi
plăti mai multe co-plă i, etc. Înainte de orice alt
după certitudini: certitudinea iubirii, a sănătă ii, a
comentariu in să vă reamintesc că în Anglia, Suedia sau
bunăstării și a vie ii veșnice. Dar la ce ne trebuiesc toate
Danemarca nu există această „libertate” de op iune, dar
aceste certitudini? Ca să ne rămână energia și timpul
au cea mai e cientă asisten ă medicală din lume. În
necesare să facem ce vrem fără vreo grijă. Nenorocirea
America libertatea e totală (po i să nici nu te asiguri!)
societă ii moderne este că certitudinile dispar încet,
dar sistemul e scump. Deci noi ce ne dorim? Asisten ă
încet din lume. Dumnezeu a murit, după cum au
medicală mai bună, echitabilă și comprehensivă, sau
descoperit ateii din cele mai vechi timpuri, dar n-au
puritate ideologică și victoria pie ei libere în sănătate?
avut curajul s-o spună cu glas tare până la Nietsche.
Rostul unei societă i private de asigurări de sănătate
Legile naturii zice au devenit din ce în ce mai complexe
este să facă bani și nu să îngrijească bolnavi! Nu
încât sunt inaccesibile majorită ii muritorilor. Singura
solidaritatea socială și ajutorul reciproc este inta lor, ci
certitudine este legea evolu iei universale, dar ea nu ne
să vândă frică. Frica de boală și de invaliditate pe care
aduce liniștea dorită ci tocmai neliniștea de care ne ferim
trebuie să le înfrun i singur și pentru care e mai bine să
din toate puterile. Desigur nici natura umană nu se prea
strângi cureaua să economisești și să le dai lor banii
schimbă, dar nici asta nu ne aduce liniștea, ci doar ne
pentru administrare. Frica de incendiu, inunda ie,
explică foamea de certitudini. În absen a lui Dumnezeu,
cutremur și malpraxis pentru care plătim cu to ii dar nu
foamea de certitudini trebuia astâmpărată cumva și
vedem niciun ban, sau în cel mai bun caz mult mai
atunci au apărut ideologiile. Ele î i livrează certitudini la
pu in decât s-a promis. Faptul că oamenii trăiesc în
pachet, dar nu precizează data expirării și nici efectele
familii și re ele sociale care intervin în ajutorul unui
adverse principale. În secolul trecut ne-am infectat cu
membru lovit de o nenorocire este un mare handicap
fascism, apoi cu comunism, dar din păcate am rămas
pentru asigurători. Sau un avantaj în măsura în care
sensibili la multe alte posibile ideologii viitoare. În
oamenii își rezolvă problemele cu prietenii și renun ă să-
ultimii ani ne-am contaminat, cel pu in la nivelul unor
și mai pretindă drepturile pentru care au plătit.
elite, de ideologia „pie ei libere”.
Să încercăm să ne imaginăm cum va cu mai multe
Cu ani în urmă, când încă mai făcem și eu câte o
societă i private de asigurări de sănătate. Vă rog ca în
subfebrilitate politică, un tânăr și vioi liberal m-a
acest demers să nu uita i premiza enun ată mai sus (cu
întrebat: „Ce trebuie să facem ca să asigurăm victoria
caractere bolduite). Voi începe direct cu concluzia:
pie ei libere în asisten a medicală?” Întâi n-am în eles
standardele de calitate ale îngrijirii bolnavilor se vor
întrebarea: „Cum adică victoria pie ei libere? Parcă noi
prăbuși. Argumentul meu ine de o experien ă pe care
doctorii luptam împotiva bolii și suferin ei și nu pentru
au trăit-o to i proprietarii de autoturisme. În ultimul an
sau împotriva victoriei pie ei libere sau a colectivismului.”
au fost mai multe scandaluri care priveau asigurările
Nu va mai relatez restul dialogului pentru că
auto. Sub presiunea concuren ei din pia ă și a dorin ei
interlocutorul meu a rămas surd și orb la argumentele
de câștig, unii asiguratori au agreat atelierele de service
mele pragmatice deși avea forma ie de medic (nu a mai
care foloseau piese falsi cate, mai ieftine, în locul celor
practicat din cauza solicitărilor epuizante ale vie ii
originale garantate de producător. Odată ce vestea s-a
publice). Problema (infec ia) însă a rămas și s-a acutizat
răspândit, au negat-o cu vehemen ă, dar nu au întârziat
brusc în ultimele luni odată cu noile propuneri de
să ofere asigurări mai scumpe pentru cei ce doreau piese
modi care a legii sănătă ii în România. De fapt este
originale. Cine a câștigat? Proprietarul de automobil
67
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
plătește mai mult de frica falsurilor; producătorul de
după introducerea acestui sistem, cheltuielile în sănătate
piese originale produce tot atât sau mai pu in și vinde
au crescut cu 40% în câ iva ani fără ca satisfac ia și
cam la același pre ; producătorul de falsuri produce și
calitatea să crească semni cativ. Pacien ii mei deja mă
vinde ceva mai pu in, iar atelierul auto încasează aceiași
întreabă: „Domnul doctor când vom începe să plătim?”
bani pentru manoperă. Singurul câștigător este
Întrebarea are însă două nuan e distincte: bătrânii,
negustorul de frică. Cred că industria publicitară ar
șomerii și săracii mă întreabă cu îngrijorarea că nu-și vor
trebui să-și schimbe sloganul: nu sexul vinde, ci frica
mai permite îngrijirea medicală obișnuită; cei din clasa
vinde cel mai bine. Se va întâmpla același lucru și în
înstărită cu nerăbdare sperând că dacă plătesc nu vor
asisten a medicală? Fără îndoială, și în plus se va duce pe
mai sta la coadă cu to i ceilal i. Voi ce le-a i răspunde,
apa Sâmbetei și bruma de solidaritate socială pe care o
dragi colegi? Noi ce ne dorim ca societate, pentru că
aveam (capitol la care societate românească stă oricum
dacă ne dorim o societate puternică ar cazul să nu mai
prost!). Dacă nu ar orbi i de ideologia pie ei libere,
stăm cu mâinile în sân și să lăsăm ideologiile să ne
reformatorii noștri ar trebuit să ne spună că în Olanda,
conducă!
Dr. Sever-Cristian Oană
68
ORIGINAL ARTICLES
DETECTAREA ANTICORPILOR ANTI LAMININ 1 DIN CLASA IgG LA
PACIENȚI CU STROKE ISCHEMIC ACUT
Manole Cojocaru1, Elena Rusu2, Inimioara Mihaela Cojocaru3, Isabela Siloşi4
1Departamentul de Fiziologie, Facultatea de Medicină, Universitatea Titu Maiorescu, Bucureşti, România,
2Departamentul de Biochimie, Facultatea de Medicină Dentară, Universitatea Titu Maiorescu, Bucureşti, România,
3Departamentul de Neurologie, Universitatea de Medicină şi Farmacie Carol Davila, Bucureşti, România, 4Departamentul
de Imunologie, Facultatea de Medicină, Universitatea de Medicină şi Farmacie, Craiova, România
Adresa pentru coresponden ă:
Cojocaru Manole
Strada omas Masaryk Nr. 5, Sector 2, Cod poştal 020983, Bucureşti, România
E-mail: mancojocaru@yahoo.com
Primit: 17.02.2014
Acceptat: 28.02.2014
Med Con March 2014 Vol 9, No 1, 69-71
Rezumat
p<0,009). ALA nu sunt speci ci bolii, dar par să e
asocia i anticoagulantului lupic
(LA), anticorpilor
Introducere: Prezen a anticorpilor anti-laminin-1
anticardiolipinici
(aCL). Valoarea predictivă negativă
(ALA) din clasa IgG poate de ni un subgrup de pacien i
pentru IgG ALA nedetectabili a fost 84%, iar valoarea
cu sindrom antifosfolipidic primar (APS) cu risc crescut
predictivă pozitivă a fost 75%.
de tromboze.
Concluzii: Rezultatele con rmă că aceşti
Obiective: Să analizăm prevalen a IgG ALA în serul
autoanticorpi sunt elibera i în circula ia sanguină după
pacien ilor cu stroke ischemic acut şi să stabilim dacă
stroke, ei pot
uşor determina i şi se corelează cu
aceşti anticorpi sunt asocia i cu evolu ia clinică.
evolu ia. Nivelurile IgG ALA cele mai crescute în ser se
Materiale şi metode: Studiul a inclus 78 pacien i
corelează cu evolu ia nefavorabilă. Prezen a IgG ALA
cu stroke ischemic acut, 46 femei şi 32 bărba i, între 46-
pare să re ecte alterarea barierei hematoencefalice
81 ani, cu vârsta medie 74,3±6,8 ani. Probele de sânge
(BHE), care favorizează accesul antigenelor sistemului
pentru determinarea IgG ALA au fost recoltate în
nervos central la celulele imunocompetente.
primele 24 de ore după debutul stroke-ului, precum şi
Cuvinte cheie: anticorpi anti-laminin-1, prevalen ă,
de la 72 martori sănătoşi, 43 femei şi 29 bărba i, între
evolu ie clinică, stroke ischemic acut
42-79 ani, cu vârsta medie 71,3±6,4 ani. IgG ALA în ser
au fost determina i folosind ELISA. Pentru analiza
Introducere
statistică, s-a folosit testul Fisher, raportul odds şi
intervalul de con den ă (IC) 95% pentru ecare caz.
In ama ia şi stresul oxidativ sunt factori importan i
Valoarea p<0,05 s-a considerat semni cativă.
care contribuie la distrugerea barierei hematoencefalice
Rezultate: Titrurile crescute de IgG ALA în ser au
(BHE) [1]. Mecanismele includ distrugerea complexelor
fost întâlnite la 58 (76%) pacien i. Nivelurile de IgG
jonc ionale interendoteliale şi inducerea de proteaze, în
ALA la pacien i cu stroke ischemic au fost semni cativ
special metaloproteinazele matriceale
(MMPs), care
mai crescute (127,32±13,42 UI/ml) comparativ cu lotul
degradează constituien ii membranei bazale vasculare
martor (26,41±1,83 UI/ml) (p<0,003). Titrul s-a corelat
[2]. Ruperea BHE este un factor important care
semni cativ cu evolu ia clinică (157,16±13,82 UI/ml;
contribuie la injurie în multe boli neurologice, inclusiv
Detection of IgG Anti-Laminin-1 Antibodies in Patients with Acute Ischemic Stroke
69
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
în stroke
[3-5]. Laminina-1 este o glicoproteină
Comitetul local de etică a aprobat protocoalele
multifunc ională a membranei bazilare. Capacitatea de
clinice, to i pacien ii şi martorii au depus consim ământul
a men ine integritatea BHE depinde de structura
informat.
corespunzătoare a membranei bazilare. Anticorpii sunt
importan i clinic în apari ia stroke-ului ischemic [6-8].
Rezultate
Obiectivele acestui studiu au fost să analizăm
prevalen a IgG ALA în probele de sânge la pacien i cu
Titruri semni cativ crescute de anticorpi au fost
stroke ischemic acut şi să stabilim dacă aceşti anticorpi
observate la 58 (76%) pacien i cu stroke ischemic acut
se asociază cu evolu ia clinică.
comparativ cu lotul martor. Nivelurile IgG ALA la
pacien ii cu stroke ischemic acut au fost semni cativ
Material şi metode
mai crescute
(limitele între
94,16-156,07 UI/mL,
valoarea medie 127,32±13,42 UI/ml) comparativ cu
Titrurile de IgG ALA în ser au fost determinate
lotul martor (limitele între 16,08-31,67 UI/ml, valoarea
imediat după internare pentru stroke ischemic acut la
medie 26,41±1,83 UI/ml) (p<0,003). Titrul s-a corelat
78 pacien i (46 femei şi 32 bărba i între 46-81 ani, cu
semni cativ cu evolu ia clinică (limitele între 134,03-
vârsta între 46-81 ani, vârsta medie 74,3±6,8 ani) şi la
188,02 UI/ml, valoarea medie 157,16±13,82 UI/ml;
72 martori sănătoşi (43 femei şi 29 bărba i, între 42-79
p<0,009). Nivelurile maxime de IgG ALA s-au corelat
ani, vârsta medie 71,3±6,4 ani).
cu severitatea şi evolu ia în primele 24 ore după debutul
Pacien ii cu
brila ie atrială în antecedente,
stroke-ului ischemic. Corela ia statistic semni cativă
valvulopatii (eviden iate la ecocardiogra e) sau boli ale
între titrurile IgG ALA şi GCS (r=0,79, p<0,009), s-a
esutului conjunctiv, au fost excluşi din studiu, de
observat corela ie statistic semni cativă între nivelurile
asemenea, cei cu boală cardiacă cu poten ial de tromboză.
IgG ALA ale grupurilor NIHSS
(16-42 puncte
-
De asemenea, criterii de excludere au fost: boli generale
prognostic nefavorabil,
7-15 puncte
- prognostic
sau psihiatrice, boli gastrointestinale in amatorii,
intermediar şi 0-6 puncte - prognostic bun) (r=0,81,
creatinina serică
>150mmol/l, guta sau insu cien a
p<0,005).
renală, sau administrarea de vitamine antioxidante,
Valoarea predictivă negativă pentru IgG ALA a fost
de citul de er. S-au folosit criteriile TOAST şi OCSP,
84%, iar valoarea predictivă pozitivă a fost
75%.
National Institutes of Health Stroke Scale (NIHSS) şi
Pacien ii cu IgG ALA în ser au prezentat manifestări
Glasgow Coma Score (GCS) la bază şi la 24 ore. Ischemia
trombotice severe.
cerebrală a fost diagnosticată folosind tehnica imagistică.
Proba de examinat (5ml) a fost recoltată în primele
Discuții
24 ore după debutul stroke-ului ischemic prin punc ie
venoasă. Serul a fost separat prin centrifugare la 4000g
Asocierea dintre IgG ALA şi stroke-ul ischemic a
timp de 5 min şi păstrat 0,5ml la -200C până în
fost analizată la
78 pacien i cu rezultatul pozitiv.
momentul efectuării tehnicii ELISA. Rezultatele au
Prezen a autoanticorpilor s-a corelat semni cativ cu
fost exprimate ca unită i arbitrare
(UI/ml). Curba ROC s-a folosit
pentru calcularea valorii cuto . S-au
folosit media
(x)±devia ia standard
(DS).
S-a folosit testul Fisher, raportul
odds şi intervalul de încredere 95%
(IC). Titrurile IgG ALA au fost
comparate folosind testul Student t.
Rela ia între prevalen a IgG ALA
şi evolu ia clinică a fost analizată
folosind testul Fisher. Valoarea p<0,05
a fost considerată semni cativ
statistică. Coe cientul de corela ie
Pearson s-a folosit pentru stabilirea
corela iei între titrurile IgG ALA şi
Figura 1. Valoarea medie a titrurilor de IgG ALA la pacien i
evolu ia clinică.
cu stroke ischemic acut comparativ cu lotul martor
70
Cojocaru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
stroke-ul ischemic. S-a demonstrat că pacien ii cu stroke
ischemic stroke:
2005 guidelines update. Stroke
ischemic acut prezintă niveluri semni cativ mai crescute
2005;36(4): 916-21.
de IgG ALA.
2.
Maas MB, Furie KL. Molecular biomarkers in stroke
Rezultatele sugerează că IgG ALA pot să aibă un
diagnosis and prognosis. Biomark Med
2009;3(4):
efect nefavorabil asupra evolu iei în stadiile precoce ale
363-83.
stroke-ului ischemic. Observa iile sugerează că IgG ALA
3.
Doyle KP, Simon RP, Stenzel-Poore MP. Mechanisms
pot responsabili de stroke ischemic, interferând cu
of ischemic brain damage. Neuropharmacology
in ama ia. Anticorpii anti-laminină-1 nu sunt speci ci
2008;55(3):310-18.
de boală, se pare că pot asocia i cu anticoagulantul
4.
Laterza OF, Modur VR, Crimmins DL, et al.
lupic
(LA), anticorpi anticardiolipinici
(aCL)
[5].
Identi cation of novel brain biomarkers. Clin Chem
Laminina, o glicoproteină multifunc ională a
2006;52(9):1713-21.
membranei bazale, constă din trei subunită i distincte,
5.
Sotgiu S, Zanda B, Marchetti B, et al. In ammatory
lan urile a, b şi g. Există cel pu in
15 izoforme de
biomarkers in blood of patients with acute brain
laminină. Lamininele prezintă activită i biologice
ischemia. Eur J Neurol 2006;13(5):505-13.
diverse, care includ favorizarea adeziunii celulare,
6.
Broughton BR, Reutens DC, Sobey CG. Apoptotic
migrarea, proliferarea şi diferen ierea, precum şi
mechanisms after cerebral ischemia. Stroke 2009;40(5):
formarea de re ea în membrana bazilară [6,9].
e331-e339.
Aceste procese biologice se petrec prin traducerea
7.
Hill MD. Diagnostic biomarkers for stroke: a stroke
semnalului, matricea celulară interac ionează mediat
neurologist’s
perspective.
Clin.
Chem
prin receptorii speci ci ai lamininei şi alte componente
2005;51(11):2001-2.
matriceale. Multe zone responsabile pentru aceste
8.
Whiteley W, Tseng MC, Sandercock P. Blood
activită i sunt localizate în domeniul carboxil-terminal
biomarkers in the diagnosis of ischemic stroke: a
globular G al lan ului a [10-13].
systematic review. Stroke 2008;39(10):2902-9.
Prezen a IgG ALA poate să de nească un subgrup de
9.
Bornstein NM, Aronovich B, Korczyn AD, Shavit S,
pacien i cu risc crescut de evolu ie nefavorabilă. În lumina
Michaelson DM, Chapman J. Antibodies to brain
acestor descoperiri, evaluarea IgG ALA ar putea utilă
antigens following stroke. Neurology 2001;56(4):529-
pentru managementul clinic al pacien ilor cu stroke
30.
ischemic acut. IgG ALA ar putea un marker serologic
10.
Zierath D, ullbery M, Hadwin J, Gee JM, Savos A,
folositor la pacien i cu variate manifestări trombotice [14].
Kalil A, Becker KJ. CNS immune responses following
experimental stroke. Neurocrit Care 2010;12(2):274-
Concluzii
84.
11.
Colognato H, Yurchenco PD. Form and function: the
Studiul a stabilit semni ca ia clinică a IgG ALA,
laminin family of heterotrimers. Dev. Dyn
demonstrând că valori crescute de IgG ALA în sânge
2000;218(2):213-34.
sunt asociate semni cativ cu stroke-ul ischemic. Pacien ii
12.
Denes A,
ornton P, Rothwell NJ, Allan SM.
cu titruri crescute de IgG ALA prezintă un risc mai
In ammation and brain injury: acute cerebral
crescut de a dezvolta manifestări trombotice. IgG ALA ar
ischaemia, peripheral and central in ammation. Brain
putea un marker serologic folositor în tratamentul
Behav Immun 2010;24(5):708-23.
precoce al pacien ilor cu manifestări trombotice. S-au
13.
Ruleva NIu, Kuzin VM, Martynov MIu, Kamchatnov
observat corela ii statistic semni cative între nivelurile
PR. Markers of in ammation, autoantibodies to
IgG ALA şi evolu ia clinică (scorul NIHSS şi GCS).
neurospeci c antigens and outcome in patients with
acute ischemic stroke. Zh Nevrol Psikhiatr Im S S
Korsakova 2004;(Suppl 12):60-5.
Referințe
14.
Aumailley M, Pesch M, Tunggal L, Gaill F, Fassler R.
Altered synthesis of laminin 1 and absence of basement
1. Adams HP, Adams R, del Zoppo G, Goldstein LB.
membrane component deposition in b1 integrin-de cient
Guidelines for the early management of patients with
embryoid bodies. J Cell Sci 2000;113Pt2:259-68.
Detection of IgG Anti-Laminin-1 Antibodies in Patients with Acute Ischemic Stroke
71
Medical Connections/Conexiuni Medicale
Declarația de conflict de interese
Medical Connections/Conexiuni Medicale (Med Con) solicită tuturor autorilor şi recenzorilor să declare
orice con ict de interese care ar putea interveni în contribu iile lor.
Con ictul de interese pentru un anumit manuscris există atunci când un participant în procesul de
recenzie inter pares (peer review) şi de publicare - autor, referent, sau editor - are legături cu activită i care
l-ar putea in uen a necorespunzător pe el sau judecata lui, indiferent dacă aceasta este sau nu afectată.
Rela iile nanciare cu industria medicală, de exemplu prin muncă salarială, consultan ă, de inere de
ac iuni, onorarii, testimoniale ca şi expert, e direct, e prin intermediul familiei, sunt de obicei considerate
a cele mai importante con icte de interese. Cu toate acestea, pot apărea con icte din alte motive, cum ar
rela iile personale, concuren a academică şi implicarea intelectuală.
Încrederea publicului în procesul de revizuire inter pares şi credibilitatea articolelor publicate depinde
în parte de cât de bine este administrat posibilul con ict de interese în timpul redactării, recenziei inter
pares şi a luării deciziilor editoriale. Părtinirea poate de multe ori identi cată şi eliminată prin aten ia
crescută asupra metodelor ştiin i ce şi concluziilor lucrării. Rela iile nanciare şi efectele lor sunt mai uşor
de identi cat decât alte con icte de interese. Participan ii la peer review şi în procesul de publicare trebuie
să-şi dezvăluie posibilele con ictele de interese, iar informa iile trebuie să e puse la dispozi ie, astfel încât
şi al ii să poată aprecia aceste efecte pentru ei înşişi.
Autori: atunci când trimit un manuscris sau o scrisoare, autorii sunt responsabili pentru recunoaşterea
şi divulgarea con ictelor nanciare şi altor con icte de interese care ar putea să le in uen eze activitatea. Ei
trebuie să recunoască în manuscris orice sprijin nanciar pentru activitate, precum şi orice alte legături
nanciare sau personale în munca lor.
Recenzorii: evaluatorii externi inter pares trebuie să dezvăluie editorilor orice con icte de interese care
le-ar putea părtini opiniile asupra manuscrisului şi ar trebui să se recuze de la recenzia anumitor manuscrise
în cazul în care cred că este oportun. Editorii trebuie să e conştien i de posibilele con icte de interese ale
recenzorilor în interpretarea recenziilor şi trebuie să judece pentru ei dacă recenzorul ar trebui să e recuzat.
Recenzorii nu trebuie să utilizeze informa iile în munca lor, înainte de publicare, pentru a-şi promova
propriile interese.
Titlul manuscrisului: ________________________________________________________
Declar că nu există con ict de interese
Declar că există următoarele con icte de interese poten iale:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Nume
Semnătura/Data
Vă rugăm trimite i acest formular semnat pe fax sau mail la sediul editorului Med Con.
Fax: +40-261-710456
Email: colmedsm@gmail.com
ORIGINAL ARTICLES
ASOCIEREA LICHENULUI PLAN BUCAL CU HEPATITA CRONICĂ CU
VIRUS C. STUDIU RETROSPECTIV
Carmen Gheorghe1, Lelia Mihai2, Ioanina Parlatescu1, Şerban ovaru1, Elena Coculescu1
1Disciplina Patologie Orală, Universitatea de Medicină şi Farmacie Carol Davila, Bucureşti, 2Catedra de Patologie
Orală, Universitatea de Medicină „Titu Maiorescu”, Bucureşti
Adresa pentru coresponden ă:
Carmen Larisa Gheorghe
Bucureşti, Strada Eforie, Nr 4-6, Etaj 3, Camera 18
Phone: 0749218099
E-mail: larisacarmen74@gmail.com
Primit: 18.02.2014
Acceptat: 28.02.2014
Med Con March 2014, Vol 9, No 1, 73-77
Rezumat
semni cativ mai mare comparativ cu pacien ii din
grupul de control 6% (8/143). Forma clinică a lichenului
Lichenul plan bucal este o afec iune dermatologică
plan la pacien ii care asociau şi infec ie cu virus hepatitic
destul de frecvent întâlnită în practica stomatologică
C a fost în 44% din cazuri cea erozivă.
curentă. S-a observant asocierea lichenului cu hepatita
Concluzii: Rezultatele ob inute au arătat o asociere
cronică cu virus C, lichenul plan ind considerat una
mai frecventă a hepatitei C la pacien ii cu lichen plan
dintre manifestările extrahepatice ale infec iei cu virus
bucal. Aceste date eviden iază necesitatea realizării
hepatitic C. Formele clinice ale lichenului plan sunt mai
screeningului pentru depistarea hepatitei C tuturor
agresive, simptomatologia acută, evolu ia cunoaşte
pacien ilor diagnostica i cu lichen plan bucal. Forma
perioade mai dese de exacerbare a leziunilor, atunci când
erozivă, acută, a lichenului plan pare să e caracteristica
este asociat cu patologie hepatică. Scopul acestui studiu
pacien ilor care asociază patologie hepatică.
este de a analiza posibilitatea asocierii lichenului plan
Cuvinte cheie: lichen plan bucal, virus hepatitic C,
bucal cu hepatita cronică C şi a investiga dacă există o
manifestari extrahepatice, leziuni erozive
anumită formă clinică a lichenului plan bucal
caracteristică acestei asocieri.
Introducere
Material şi metodă: am realizat un studiu
retrospectiv analizând şele de observa ie a
380 de
Lichenul plan bucal (LPB) este o maladie cronică,
pacien i consecutivi, diagnostica i cu lichen plan bucal
nein amatorie, cu afectare cutaneo-mucoasă. Leziunile
în serviciul clinic al Disciplinei de Patologie Orală,
clinice pot
întâlnite cel mai frecvent la nivelul
Universitatea de Medicină şi Farmacie Carol Davila,
epiteliului malpighian al tegumentului şi mucoasei
Bucureşti, între anii 2007-2010. La aceşti pacien i s-au
orale, dar şi pe mucoasa esofagiană, genitală sau pe scalp
urmărit rezultatele testelor serologice pentru markerii
[1,2]. În cazuri rare leziunile pot să apară la nivelul
hepatitei C şi forma clinică a leziunilor orale în
unghiilor. Complica iile acestor cazuri pot distrugerea
momentul prezentării.
ireversibilă a matricei unghiale (sau rădăcina unghiei),
Rezultate: Pacien ii din grupul de studiu au
cu sub ierea sau chiar pierderea unghiei [1]. Prevalen a
prezentat o asociere de 18% (50/273) cu hepatita C,
LPB în rândul popula iei generale este variabilă, studii
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
73
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
recente raportând valori de 0,5-2,5% [3]. Sunt afectate
privitoare la sexul, vârsta şi mediul de provenien ă al
cu predilec ie femeile adulte în decadele 5-6 de via ă şi
pacien ilor,
antecedentele
heredo-colaterale
şi
numai în mod excep ional copiii [3,4]. Etiopatogenia
patologice, motivele prezentării, simptomatologia
LPB este şi astăzi un subiect intens discutat. În prezent
acuzată şi vechimea afec iunii orale. De asemenea, au
se consideră că reac iile imunologice au un rol important
fost urmărite referirile la stresul cronic asociat cu debutul
în declanşarea mecanismului ziopatologic. Antigenele
bolii, aspectul clinic la momentul prezentării şi numărul
modi cate stimulează celulele bazale şi celulele
de zone afectate. Dintre investiga iile paraclinice
Langerhans declanşând astfel o cascadă de reac ii
realizate, a fost urmărită în special determinarea Ac anti
imunologice, care în nal vor determina apoptoza
VHC, prin metoda ELISA genera ia II-III. În cazul
keratinocitelor bazale
[4,5]. De cele mai multe ori
rezultatelor pozitive au fost recomandate teste de
leziunile orale au aspect clinic şi localizare tipică. În
con rmare, metoda Imunoblot, care determină
mod obişnuit LPB prezintă leziuni keratozice, atro ce,
anticorpii Ig G speci ci anti-VHC.
erozive sau mai rar buloase [6]. Simptomatologia este
Astfel a fost constituit lotul de studiu format din
acuzată de pacien i, mai ales în cazurile grave, întinse, în
273 pacien i diagnostica i cu LPB.
care predomină leziunile atro ce sau erozive.
Diagnosticul de LPB a fost stabilit pe criterii clinice
Dinamismul şi variabilitatea în timp a leziunilor clinice
în principal, ind luate în considerare numai cazurile cu
sunt in uen ate în mare parte de către vechimea şi
aspect clinic tipic şi localizare caracteristică a leziunilor.
gradul de activitate al bolii [2,4].
Con rmarea histologică a diagnosticului clinic a
Evolu ia lichenului plan este cronică, pe parcursul
fost făcută în
205 cazuri
(75%) care nu au avut
căreia se succed perioade de exacerbare a leziunilor orale
modi cări ale constantelor paraclinice hematologice şi
cu perioadele de remisiune în care simptomatologia este
nu au avut nicio contraindica ie de ordin general pentru
mult diminuată. Spre deosebire de formele cutanate,
efectuarea biopsiei. Ca investiga ii complementare de
LPB are o evolu ie mult mai îndelungată, pe parcursul
diagnostic în
2 cazuri s-a realizat şi examenul de
mai multor ani şi având un răspuns terapeutic
imuno uorescen ă directă, iar în 3 cazuri examenul de
nesatisfacător în unele cazuri
[4]. Asocierea cu
imunohistochimie.
hepatopatiile cronice, în special cu hepatita cronică C
Grupul control a fost constituit din 143 pacien i
este o chestiune bine documentată, existând ipoteza că
fără modi cări sau leziuni ale mucoasei orale la
virusul hepatitei C
(VHC) ar putea implicat în
momentul examinării, care s-au prezentat în serviciul
patogeneza LPB [7,8,9]. Mecanismele implicării VHC
nostru pentru tulburări de percep ie ale mucoasei orale
în patogenia lichenului plan sunt în prezent explicate
fără corespondent clinic, simptomatologie sugestivă
printre altele, prin replicarea VHC nu numai în
pentru diagnosticul de algie bucală nespeci că. La
hepatocit ci şi în celulele extrahepatice, producând
pacien ii din grupul control au fost urmărite date
afectarea şi liza acestora datorită efectului citopatic [10].
referitoare la vârstă şi sex şi rezultatele analizelor de
Studiul îşi propune să investigheze posibilitatea asocierii
determinare a prezen ei Ac anti VHC.
LPB cu hepatita cronică cu virus C şi să analizeze
formele clinice pe care aceşti pacien i le prezintă în
Rezultate
momentul examinării.
Grupul de studiu a fost compus din 273 de pacien i
Material şi metode
cu vârsta cuprinsă între 20 şi 95 ani (media vârstei de
56,87). Dintre aceştia, 219 pacien i (80%) au fost femei
A fost realizat un studiu retrospectiv analizând
şi 54 (20%) bărba i.
datele consemnate în foile de observa ie a
380 de
În ceea ce priveşte antecedentele heredocolaterale, 5
pacien i consecutivi, diagnostica i cu LPB în serviciul
pacien i au relatat că rudele de gradul 1 au prezentat
clinic al Disciplinei de Patologie Orală, Universitatea de
istoric medical de lichen plan cutanat sau oral, 1 pacient
Medicină şi Farmacie Carol Davila, Bucureşti, între anii
a prezentat istoric familial de lupus şi 8 pacien i au avut
2007-2010.
cazuri de carcinoame ale mucoasei tubului digestiv sau
Criteriile de includere în studiu au fost reprezentate
ale cavită ii orale la rudele apropiate.
de: pacien i diagnostica i cu LPB, teste pentru
Un număr de 156 (57%) de pacien i au a rmat că
determinarea anticorpilor anti-virus hepatitic C (Ac anti
debutul LPB a coincis cu un stres emo ional puternic,
VHC).
89 (33%) pacien i au negat această asociere şi 28 (10%)
Din foile de observa ie ale pacien ilor selecta i
pacien i nu au putut preciza dacă au remarcat o legătură
pentru acest studiu au fost extrase date generale
de tip cauză-efect între cele două aspecte.
74
Gheorghe et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
În ceea ce priveşte intervalul de timp scurs de la
sesizarea leziunilor orale, acesta a avut valori variabile.
Astfel
71(26%) de pacien i s-au prezentat la prima
consulta ie în mai pu in de 3 luni de la debutul acuzelor,
45 (16%) pacien i după 3-6 luni, 52 (19%) pacien i au
fost diagnostica i cu LPB după aproximativ 1 an de la
debut, 58 (21%) pacien i după 1-5 ani, iar 23 (8%) de
pacien i acuzau prezen a simptomatologiei de peste 5
ani. În 9% din cazuri (24 pacien i) nu a putut stabilit
cu exactitate momentul debutului, pacien ii neputând
preciza acest aspect.
În urma determinărilor Ac anti VHC în grupul de
studiu,
50
(18%) pacien i au prezentat rezultate
Figura 1. Prezen a semni cativă din punct de vedere
pozitive, iar 223 (82%) pacien i au prezentat rezultate
statistic a Ac anti VHC în grupul de studiu
negative (Figura 1).
În urma analizei de subgrup s-a urmărit distribu ia în
ceea ce priveşte vârsta, sexul, simptomatologia acuzată,
forma clinică şi numărul de zone afectate la pacien ii cu
LPB care asociază hepatita cronică cu VHC. Astfel s-au
ob inut următoarele rezultate: grupul compus din cei 50
de pacien i care au fost diagnostica i cu LPB şi infec ie cu
VHC a fost format din 46 (92%) femei şi din 4 bărba i
(8%). În ceea ce priveşte vârsta, aceasta a fost cuprinsă în
intervalul 41-83 de ani, cu o medie a vârstei de 63 de ani.
Formele clinice observate la pacien ii cu hepatită cu virus
C asociată sunt predominant erozive în 22 (44%) cazuri,
urmată în ordinea frecven ei de formele keratozice în 18
(36%) cazuri, forme atro ce în 8 (16%) situa ii şi numai
2
(4%) cazuri de forme predominant buloase. În
Figura 2. Pacien ii din grupul control au un risc
concordan ă cu gravitatea formei clinice, simptomatologia
mai scăzut de a infecta i cu VHC
acuzată de pacien i a avut grade diferite de intensitate, dar
a fost prezentă la 45 (90%) pacien i, în timp ce numai 5
(10%) cazuri au fost asimptomatice. În ceea ce priveşte
Tabelul I: Leziunile clinice predominante la pacien ii
localizarea leziunilor clinice, la pacien ii care au asociat
cu LPB şi hepatita cronică cu VHC
hepatita cronică cu virus C, au predominat formele acute,
Forma clinică
Număr cazuri
Procent
întinse, cu peste 4 zone interesate în 27 (54%) cazuri.
Erozivă
22
44%
Leziunile orale au fost prezente la nivelul mucoasei jugale
bilateral la 10 (20%) pacien i, 3 zone afectate au fost
Keratozică
18
36%
descrise în
11
(22%) cazuri, în timp ce afectarea
Atro că
8
16%
unilaterală a fost observată numai în 2 (4%) cazuri.
Buloasă
2
4%
Analizând structura grupului control inclus în acest
studiu, s-a remarcat structura acestuia în ceea ce priveşte
reparti ia pacien ilor în func ie de sexul acestora: 98
(8/143, 6%). În ceea ce priveşte forma clinică, leziunile
(69%) de pacien i au fost femei şi 45 (31%) bărba i, iar
erozive sunt predominante la pacien ii diagnostica i cu
media vârstei a fost calculată la valoarea de 55,95. În
lichen plan bucal care prezintă hepatita C ca patologie
urma analizării rezultatelor ob inute la determinarea Ac
asociată (Tabelul I).
anti VHC s-a observat că 135 (94%) au avut rezultate
negative, iar 8 (6%) au fost seropozitivi (Figura 2).
Discuții
Comparând rezultatele ob inute, se observă că
pacien ii diagnostica i cu LPB din grupul de studiu au
Corela ia dintre LPB şi hepatopatiile cronice, în
un risc semni cativ mai mare de a asocia infec ia cu
special cu hepatita cronică cu VHC a fost remarcată
VHC (50/273, 18%) decât pacien ii din grupul control
prima dată în 1978 de către Rebora, iar de atunci au fost
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
75
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
realizate
numeroase studii pe această temă.
LPB, numai în 5% din determinari Ac anti VHC au fost
Particularitatea VHC de a avea tropism atât pentru
prezen i. Astfel, prevalen a infec iei cu VHC la pacien ii
celula hepatică cât şi pentru limfocite îi conferă acestuia
cu LPB a fost mai mare în grupul de studiu decât în
un caracter ubicuitar, consecin a ind inciden a mai
grupul control. Aceste rezultate justi că investigarea unei
mare a manifestărilor autoimune extrahepatice la
poten iale infec ii cu VHC la pacien ii cu LPB [15].
pacien ii cu infec ie cronică cu VHC.
La polul opus sunt rezultatele studiilor din Anglia
Rezultatele ob inute în studiile clinice realizate
care nu au găsit nicio legătură între cele două afec iuni
abordând această temă au fost contradictorii, ind în
[16].
mare parte dependente de zona geogra că în care s-au
În ceea ce priveşte forma clinică, unele studii arată
efectuat şi mai pu in de vârsta sau sexul pacien ilor.
rezultate similare studiului nostru. Astfel, Carrozzo şi
Acest fapt este explicat de inciden a variabilă a infec iei
colab., la pacien ii care asociază infec ie cronică cu
cu VHC pe glob, existând zone care prezintă din acest
VHC, au găsit la 58,8% dintre ei forma erozivă a LPB
punct de vedere un risc endemic scăzut (America de
[12]. Tot forma erozivă de LPB a fost observată şi într-
Nord, Europa de Nord), risc endemic mediu (Sudul şi
un alt studiu realizat în Italia [17], în timp ce al i autori
Sud-Estul Europei, America de Sud, America Centrală,
au găsit ca formă clinică predominantă forma reticulară
Australia, Europa Centrală şi de Est, Africa Subsahariană,
[18]. Pe de altă parte, în studiul realizat în popula ia din
sudul Asiei), sau ridicat
(nordul Africii, Orientul
Israel nu s-a găsit nicio corela ie între asocierea LPB cu
Mijlociu, Asia Centrală şi de Est) [11].
infec ia cronică cu VHC şi o anumită formă clinică a
Studiul nostru a prezentat
273 de pacienti
afec iunii orale [14].
diagnostica i cu LPB la care s-au determinat Ac anti
VHC şi la care s-a urmărit descrierea clinică a leziunilor
Concluzii
orale în momentul prezentării. Rezultatele ob inute au
arătat o seropozitivitate mult mai mare pentru markerii
Este recomandată dispensarizarea atentă a
hepatitei C la pacien ii incluşi în grupul de studiu
pacien ilor cu LPB care asociază hepatita cronică cu
comparativ cu grupul control. De asemenea, forma
VHC, deoarece s-a observat că în această situa ie
clinică predominantă a fost cea erozivă la pacien ii care
evolu ia cunoaşte perioade de exacerbare a leziunilor
asociază infec ia cronică cu VHC, iar simptomatologia a
clinice în cazul decompensării bolii hepatice de fond.
fost prezentă la majoritatea cazurilor.
Urmărirea statusului func iei hepatice este
Studiile din literatura medicală de specialitate arată
importantă, deoarece înrăută irea hepatitei se înso eşte
rezultate similare studiului nostru în Spania, Italia sau
de recăderi ale lichenului plan.
Japonia, ări care prezintă un risc endemic mediu pentru
De cele mai multe ori pacien ii cu LPB care asociază
infec ia cu VHC la fel ca şi ara noastră. Astfel Carrozzo
şi infec ie cu VHC prezintă forme acute, erozive, înso ite
şi colab., realizând un studiu prospectiv pe un lot de 70
de o simptomatologie importantă care produce tulburări
de pacien i diagnostica i cu lichen plan bucal şi un lot
func ionale pacientului şi îi afectează via a personală.
control tot de 70 de pacien i concordant ca vârstă şi sex
Rezultatele studiului realizat arată posibilitatea ca
cu lotul de studiu, au observat o prevalen ă mai mare a
virusul hepatitei C să e implicat în patogeneza
infec iei cu VHC în grupul de studiu comparativ cu
lichenului plan bucal, eviden iind importan a
lotul control [12]. Un alt studiu clinic condus de catre
screeningului pentru detectarea prezen ei Ac anti VHC
Lodi în Italia în 2004, care a inclus 581 pacien i, 303 în
la pacien ii diagnostica i cu LPB.
grupul de studiu şi 278 în grupul control, a ob inut
Men iune: Această lucrare este efectuată în cadrul
următoarele rezultate: 19,1% din pacien ii cu lichen
Programului Opera ional Sectorial pentru Dezvoltarea
plan bucal au prezentat şi Ac anti HCV pozitivi, în timp
Resurselor Umane (POSDRU) 2007-2013, nan at din
ce în grupul control procentul pacien ilor cu Ac anti
Fondul Social European şi Guvernul României prin
VHC prezen i a fost de numai 3,2% [13].
contractul nr. POSDRU/107/1.5/S/82839
Un studiu similar realizat în popula ia din Israel a
arătat rezultate comparabile [14].
Într-o cercetare realizată în Spania, Bagan şi colab.
Referințe
au investigat un grup format din
100 pacien i
diagnostica i cu LPB la care s-au determinat Ac anti
1. Eisen D. e evaluation of cutaneous, genital, scalp,
VHC şi au găsit în 23% din cazuri rezultate pozitive. În
nail, esophageal and ocularinvolviment in patients with
grupul control compus tot din
100 pacien i clinic
oral lichen planus. Oral Surg Oral Med Oral Pathol
sănătoşi, fără leziuni sugestive pentru diagnosticul de
Oral Radiol Endod 1999;88(4):431-6.
76
Gheorghe et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
2.
Scully C, Carozzo M. Oral mucosal disease: Lichen
New estimates of age-speci c antibody to HCV
planus. Br J Oral Maxillofac Surg 2008;46(1):15-21.
seroprevalence. Hepatology 2012; Nov 21.
3.
McCartan BE, Healy CM. e reported prevalence of
12.
Carrozzo M, Gandolfo S, Carbone M, Colombatto P,
oral lichen planus; a review and critique. J Oral Pathol
Broccoletti R, Garzino-Demo P, Ghisetti V. Hepatitis
Med 2008;37(8):447-53.
C virus infection in Italian patients with oral lichen
4.
Tovaru S, Tovaru M, Costache M, Demarossi F.
planus: a prospective case-control study. J Oral Pathol
Medicină şi patologie orală. Vol I. Q Med Publishing,
Med 1996;25(10):527-33.
2008.
13.
Lodi G, Giuliani M, Majorana A, Sardella A, Bez C,
5.
Sugerman PB, Savage NW, Walsh LJ, et al. e
Demarosi F, Carrassi A: Lichen planus and hepatitis C
pathogenesis of oral lichen planus. Crit Rev Oral Biol
virus: a multicentre study of patients with oral lesions
Med 2002;13(4):350-65.
and a systematic review. Br J Dermatol 2004;151:1172-
6.
Crispian Scully. Oral and Maxillofacial Medicine. e
81.
Basis of Diagnosis and Treatment. Second edition,
14.
Yarom N, Dagon N, Shinar E, Gorsky M. Association
Churchill Livingstone Elsevier, 2008.
between hepatitis C virus infection and oral lichen planus
7.
Gheorghe C, Mihai L, Parlatescu I, Tovaru S.
in Israeli patients. Isr Med Assoc J 2007;9(5):370-2.
Afec iuni ale mucoasei orale asociate cu infec ia cu virus
15.
Bagán JV, Ramón C, González L, Diago M, Milián
hepatitic C: lichenul plan bucal. Med Con
MA, Cors R, Lloria E, Cardona F, Jiménez Y.
2013;41(8):101-4.
Preliminary investigation of the association of oral lichen
8.
Lodi G, Pellicano R, Carrozzo M. Hepatitis C virus
planus and hepatitis C. Oral Surg Oral Med Oral
infection and lichen planus: a systematic review with
Pathol Oral Radiol Endod 1998;85(5):532-6.
meta-analysis. Oral Dis 2010;16(7):601-12.
16.
Ingafou M, Porter SR, Scully C, Teo CG. No evidence
9.
Lodi G, Giuliani M, Majorana A, Sardella A, Bez C,
of HCV infection or liver disease in British patients with
Demarosi F, Carrassi A. Lichen planus and hepatitis C
oral lichen planus. Int J Oral Maxillofac Surg
virus: a multicentre study of patients with oral lesions
1998;27(1):65-6.
and a systematic review. Br J Dermatol
17.
Gandolfo S, Carbone M, Carrozzo M, Gallo V. Oral
2004;151(6):1172-81.
lichen planus and hepatitis C virus (HCV) infection: is
10.
Prabhu S, Pavithran K, Sobhanadevi G. Lichen planus
there a relationship? A report of 10 cases. J Oral Pathol
and hepatitis c virus (HCV)-is there an association? A
Med 1994;23(3):119-22.
serological study of
65 cases. Indian J Dermatol
18.
Mignogna MD, Lo Muzio L, Lo Russo L, Fedele S,
Venereol Leprol 2002; 68(5):273-4.
Ruoppo E, Bucci E. Oral lichen planus: di erent
11.
Mohd Hana ah K, Groeger J, Flaxman AD, Wiersma
clinical features in HCV-positive and HCV-negative
ST. Global epidemiology of hepatitis C virus infection:
patients. Int J Dermatol 2000;39(2):134-9.
The Association of Oral Lichen Planus with Chronic Hepatitis C. Retrospective Study
77
Scrisoare de informare
Având în vedere activită ile revistei Medical Connections/Conexiuni Medicale privind recenzia şi
editarea articolului mai jos numit, efective odată cu acceptarea acestuia de către Medical Connections/
Conexiuni Medicale (la care se face referin ă în continuare ca Med Con), autorul (autorii) atribuie prin
prezenta către Med Con, reprezentan ilor legali, succesorilor şi mandata ilor ei, toate drepturile de
publicare şi ecare şi oricare drept privind articolul în întreaga lume, în orice limbă şi în orice mediu, chiar
şi ca lucrare audiovizuală, colectivă, compila ie, lucrare derivată, lucrare în comun, operă literară,
înregistrare audio, în imagini, gra că, operă de artă vizuală, program de calculator, sau orice alt mediu
existent acum sau care va deveni ulterior uzual, inclusiv drepturile de autor şi dreptul de a înregistra
dreptul de autor, precum şi dreptul de a asigura orice reînnoire, reeditare şi extinderea unor astfel de
drepturi de autor în România sau în orice ară străină. Autorul (Autorii) pot solicita permisiunea de a
reutiliza manuscrisul sau por iuni din acesta. Astfel de cereri trebuie să e în scris, iar permisiunea dată de
Med Con nu va refuzată în mod nejusti cat. Autorul (Autorii) desemnează Med Con ca reprezentant
legal al acestuia (acestora) pentru a întocmi orice documente pe care Med Con le consideră necesare
pentru a înregistra oricare dintre aceste garan ii la o ciul de copyright românesc sau din alte ări. Autorul
(Autorii) garantează de asemenea către Med Con că articolul este lucrarea originală a autorului (autorilor),
cu excep ia materialelor provenite din domeniul public, iar fragmente din alte lucrări pot incluse doar cu
acordul prealabil scris al titularilor drepturilor de autor, că articolul nu a fost publicat anterior, nu a fost
prezentat, sau acceptat pentru publicare în altă parte, că autorul (autorii) nu au nicio rela ie, nanciară sau
de altă natură, cu orice producător sau distribuitor de produse evaluate în această lucrare, sau, dimpotrivă,
orice astfel de rela ie a fost dezvăluită într-o notă de subsol la articol, sau că această cerin ă este irelevantă
pentru lucrare.
Titlul manuscrisului: ________________________________________________________
Nume:
Semnătură/Data:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Vă rugăm trimite i pe fax +40-261-710456 această scrisoare la sediul editorului Med Con.
ORIGINAL ARTICLES
ASPECTE CLINICE ŞI TOMOGRAFICE CT ALE COMPLICAȚIILOR
PANCREATITEI ACUTE
Gheorghe Nicolae Sârbu1, Lorant Kiss1, Alina Bereanu1, Roland Kiss1, Dan Maniu2
1Clinica Chirurgie I, 2Departamentul de Radiologie, Spitalul Clinic Jude ean de Urgen ă Sibiu, Universitatea Lucian
Blaga, Sibiu
Adresa pentru coresponden ă:
Sârbu Gheorghe Nicolae
Spitalul Clinic Jude ean de Urgen ă Sibiu
B-dul Corneliu Coposu nr.2-4, Cod 550245, Romania, Sibiu
E-mail: dr.sarbu@yahoo.de
Primit: 30.01.2014
Acceptat: 27.02.2014
Med Con March 2014, Vol 9, No 1, 79-86
Rezumat
Introducere
Severitatea pancreatitei acute este clasi cată în cinci
Pancreatitele acute sunt un grup de leziuni
grade (0-4), pe baza imaginii tomogra ei computerizate
reversibile caracterizate prin in ama ii ale pancreasului,
(CT), în timp ce extensia necrozei pancreatice se
variind ca severitate de la edem şi necroza esutului gras,
măsoară prin CT cu contrast. Jumătate din decesele
până la necroza parenchimului cu hemoragii severe.
precoce se produc în primele 14 zile, pe când decesele
Majoritatea episoadelor de pancreatită acută sunt
tardive se produc pâna la
3 luni, prin insu cien ă
uşoare şi limitate, necesitând spitalizare de scurtă durată.
multiorganică, având originea primară în răspunsul
Totuşi 20% dintre pacien i dezvoltă forma severă, cu
in amator acut sistemic (SIRS) şi în infec ia necrozei
unele complica ii locale şi extrapancreatice caracterizate
pancreatice.
prin apari ia precoce şi persisten a hipervolemiei şi
Scorul precoce al gradului de severitate CT se
insu cien ei pluriorganice [1].
corelează bine cu apari ia complica iilor, a sepsisului şi
Necroza pancreatică este cea mai severă complica ie
cu procentul de mortalitate.
locală deoarece este frecvent asociată cu infec ii
Avantajele CT-ului cu substan ă de contrast în
pancreatice. Inciden a ratei mortalită ii la necroza sterilă
stadializarea pancreatitei acute se bazează pe capacitatea
şi infectată este de
10%, respectiv 25%. Severitatea
CT-lui de a arăta morfologia glandei şi afectarea
pancreatitei acute este clasi cată în 5 stadii pe scanarea
esuturilor retropancreatice, peripancreatice.
tomogra că computerizată
(CT) fără substan ă de
Extensia necrozei se cuanti că în sub 30%, până la
contrast şi după gradul necrozei măsurate prin scanare
50%, sau peste
50% din glanda pancreatică, iar
cu substan ă de contrast [2].
acurate ea generală a CT-lui în decelarea necrozei,
Complica iile care au loc în timpul unui episod de
con rmată chirurgical, a fost de 87%.
pancreatită acută sunt responsabile pentru mortalitatea
Tratamentul pacien ilor cu pancreatită acută se
între
2% şi 10%, raportată pentru această afec iune
bazează pe stabilirea precoce a severită ii bolii.
[3,4,5,6].
Cuvinte cheie: pancreatită acută, complica ii
Complica iile sistemice precoce asociate cu
precoce, complica ii tardive
insu cien a multiplă de organ (MSOF) sunt responsabile
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
79
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
pentru rata mortalită ii între 20% şi 50%, raportate
Prezentarea clinică şi nivelul de insu cien ă al
pentru pancreatita acută
[7,8,9]. Primele
2-3 zile
sistemelor diferă de la caz la caz, în corela ie cu severitatea
cuprind complica iile precoce cu manifestări clinice ale
bolii în stadiile incipiente.
sistemului cardiovascular, pulmonar, renal şi metabolic.
Criterile de incluziune pentru pancreatita acută şi
Perioada intermediară de 2-5 săptămâni cuprinde
formele sale severe au fost: durere violentă, simptomele
manifestările infec iilor locale, retroperitoneale, a
SIRS, nivelul amilazei serice mărit de cel pu in 3 ori,
necrozei infectate, a abcesului, a pseudochisturilor,
CT pozitiv cu patologii intra- sau extraperitoneale,
complica ii biliare şi gastrointestinale. Perioada tardivă,
proteina C-reactivă
≥60 sau ≥250mg/L, insu cien ă
luni-ani, cuprinde complica iile vasculare şi hemoragice,
renală cu creatinina >180 µmol/L.
ascita pancreatică.
În stadiul precoce prezentarea clinică şi gradul de
Scopul lucrării este prezentarea unei strategii
insu cien ă sistemică a fost corelat cu complica ii
diagnostice şi a unei conduite terapeutice adaptate
cardiace, pulmonare, renale şi modi cări metabolice.
severită ii ecărui caz.
La complica iile intermediare elementele controlate
au fost necroza pancreatică infectată cu complica ii
Materiale şi metode
locale şi sistemice, complica iile gastrointestinale şi
biliare, precum şi implicarea organelor solide.
În perioada martie
2002-martie
2012 au fost
La complica iile tardive s-au examinat modi cările
interna i în sec ia Chirurgie I a Spitalului Clinic de
vasculare, hemoragice şi ascita pancreatică.
Urgen ă Sibiu 103 pacien i (60 bărba i şi 43 femei) cu
predispozi ie pentru pancreatită acută severă.
Rezultate
Etiologia pancreatitei a fost metabolică (alcoolism) în
41 cazuri (31 bărba i şi 10 femei), mecanică în 46 cazuri
În stadiul precoce: manifestările sistemice cu
(22 bărba i şi 24 femei), vasculară în 5 cazuri (3 bărba i şi
complica ii sistemice au fost in ltrat pulmonar
2 femei), infec ioasă în 11 cazuri (4 bărba i şi 7 femei).
detectabil/efuziuni pleurale
(41 cazuri), sindrom de
Figura 1. Necroză pancreatică cu dezvoltarea unui pseudochist, ileus şi in amarea colonului la un bărbat
de 38 de ani. A-La internare, CT indică pancreas mărit cu in amare peripancreatică, lichid (N=necroză,
P=pancreas, S=stomac), B-Necroză liche ată 9 zile mai târziu cu o colec ie lichidiană par ial încapsulată
în bursa omentală, C-Anse dilatate ale intestinului mic cu colon transvers haustral (S=Intestinul sub ire
T=Colon transvers), D-5 săptămâni mai târziu, un pseudochist pe deplin încapsulat în bursa omentală,
necroză liche ată la nivelul istmului pancreatic (D=Duoden, N=necroză, P=pseudochist, S=Stomac)
80
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
detresă acută respiratorie (SDRA) (21 cazuri), oligurie
Tabelul I. Complica iile sistemice
(82 cazuri), hiperglicemie
>200mg%
(55 cazuri),
şi manifestările pancreatitei acute
hipocalcemie
<8mg% (39 cazuri), nivelul amilazei
Leziuni
%
serice, proteina C-reactivă, creatinina (Tabel I).
In ltrat pulmonar detectabil/efuziuni
Mortalitatea în stadiul precoce: în acest studiu în 6
40%
pleurale
cazuri (47%) dintre decese au avut loc la un interval
SDRA
20%
mediu de 8 zile (1-11 zile), secundar MSOF, în timp ce
Oligurie
80%
la 7 cazuri (53%) a survenit tardiv la un interval mediu
Hiperglicemie >200mg%
>50%
de 55 de zile (18-80 zile) secundar necrozei pancreatice
Hipocalcemie <8mg%
38%
infectate sau septicemiei retroperitoneale difuze.
Complica iile intermediare au apărut între săptămâna a
doua şi a cincea după un atac de pancreatită acută.
În acest grup de studiu decesul a apărut la 1 caz
Tabelul II. Bacteriile incriminate
(8%) dintre pacien ii cu necroză focală
(<30% din
în infec iile pancreatice
pancreas), 4 cazuri (25%) din persoanele cu necroză
Bacterii
Număr de cazuri (%)
între 30%-50% şi la 8 cazuri (52%) din pacien ii cu
E. Coli
14 (36,84%)
necroză >50%.
Enterobacter
10 (26,32%)
În studiul nostru, infec ia bacteriană secundară a
Klebsiella
9 (23,68%)
apărut la 70% din pacien ii cu pancreatită necrotică.
Anaerobi
5 (13,16%)
Necroza a fost prezentă la 20% din pacien ii cu necroză
Total
38 (100%)
secundară infectată de
10%. La evolu ia esutului
necrotic steril, lichi erea are loc în primele 2-3 zile de la
eveniment. În această situa ie, imagistica CT prezintă o
zonă de modi care scăzută care demarchează esutul
viabil de cel necrotic.
Observăm că esutul necrotic steril are tendin a să se
liche eze în primele
2-3 zile de evolu ie, când pe
imaginea CT se depistează modi cări, demarcând
esutul viabil de cel necrotic (Figura 1).
La necroza infectată, cele mai des incriminate
bacterii sunt organismele gram-negative de origine
intestinală (Tabel II).
La pacien ii cu necroză, infec ia secundară a fost
prezentă între săptămâna a doua şi a patra de evolu ie
Figura 2. Necroză pancreatică infectată,
(Figura 2).
pe imagistica CT peste 50% este necroză
Detectarea gazelor la 12%-18% din cazuri (Fig. 2)
cu liche ere încapsulată, cu bule de aer
indică necroză.
Abcesul pancreatic survine în 3 cazuri (3%) din cele
cercetate (Figura 3), de obicei la 3-4 săptămâni după
debutul pancreatitei acute.
Majoritatea pseudochisturilor care se dezvoltă după
un atac de pancreatită acută sunt asociate cu necroză,
dezvoltându-se la locul acesteia (Figura 1-4).
40% dintre pseudochisturile acute au avut o
resorb ie spontană şi o rată a complica iilor de 20%, în
timp ce pseudochisturile prezente pentru mai mult de
12 săptămâni nu aveau tendin a să se resoarbă şi au fost
asociate cu o rată a complica iilor de 65%.
Chisturile cu un diametru peste
6 cm necesită
Figura 3. Imagistica CT. Abces pancreatic la 5
tratament chirugical la mai mult de 60%, cele sub 6 cm
săptămâni după pancreatită. Colec ie lichidiană
(40%) şi pseudochisturile acute sub 5 cm în mărime
eterogenă anterioară corpului şi cozii
observate la pacien i asimptomatici la sfârşitul unui
pancreasului. Ductul pancreatic prezintă distensie
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
81
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Figura 4. Pseudochist pancreatic secundar necrozei.
A - Necroză cu liche ere la nivelul cozii, B - Pseudochist mare care are protuberan ă înspre stomac
Figura 5. Pseudochist care comunică cu ductul pancreatic, A-Cu imagine CT de glandă mărit şi
peripancreatită, B-După externarea din spital, un examen CT după 2 săptămâni mai târziu indică o
colec ie reziduală, C-6 luni mai târziu pacientul prezintă durere abdominală. CT arată un pseudochist
în creştere, D-Punc ia transgastrică cu stulogra e indică comunicarea cu canalul Wirsung
episod de pancreatită acută sunt abordate conservator,
după un episod de pancreatită acută. În studiul nostru,
cu un control CT de urmărire (Figura 5).
compromiterea lumenală arterială a dus la ischemia
La 16 cazuri, stomacul, duodenul, colonul transvers
segmentară colonică sau a intestinului sub ire proximal
sunt implicate în spasmul localizat la exura splenică a
şi infarct în 4 cazuri (Figura 9).
colonului. Aceasta explică distensia semni cativă a
Ascite de volum mic, tranzitorii, identi cate pe
colonului transvers proximal plin de aer (Figura 6).
imagini CT au fost relativ frecvente la 10 cazuri dintre
Dintre organele solide, implicarea splenică a fost cea
pacien ii cu pancreatită acută. Ascita masivă pancreatică
mai comună datorită topogra ei între coada pancreasului
poate să apară precoce, sau după câteva episoade de
şi hilul splenic (Figura 7, 8).
pancreatită acută. În studiul nostru, pacien ii cu ascită
Majoritatea complica iilor grave au tendin a de a se
masivă au avut circumferin a abdominală mărită în 24
manifesta târziu, în decurs de câteva luni până la ani de cazuri, durere abdominală în 24 de cazuri, scădere în
82
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Figura 6. A - Pancreas cu mărime normală, cu unele colec ii lichidiene peripancreatice (D=duoden,
S=stomac, P=pancreas), B - Colonul transvers este umplut cu aer şi destins, C - Filmul abdominal
arată distensia colonului transvers
Figura 7. Hemoragie intrasplenică şi subcapsulară
Figura 8. Splenomegalie şi varice gastrice
(H=hemoragie, S=splină, P=pancreas)
cu 2 episoade de pancreatită. Splină mărită masiv
cu infarct periferic
Figura 9. Colon drept infarctat în pancreatită acută, A-Imaginea CT arată pseudochist cu necroză
pancreatică la 6 săptămîni după pancreatita acută, B-o lună mai târziu, CT arată pneumatoză tardivă
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
83
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
greutate în 22 de cazuri, precum şi grea ă sau vărsături
[34,35,36]. Prezen a zonelor de pancreas solid sau
ocazionale în 2 cazuri.
poten ial liche at slab delimitate pe CT nu este
su cientă pentru diagnosticul infec iei, lucru demonstrat
Discuții
în studiul nostru în Figura 2, fapt con rmat şi de studiile
lui Kelly şi colab. [37].
Complica iile precoce asociate cu insu cien a
În cazurile studiate, detectarea bulelor de gaz în
pluriorganică
(primele
2-3 zile cu SIRS) sunt
esutul necrotic la aproximativ 12% până la 17% dintre
responsabile pentru o mortalitate de 20-50% [10,11,12].
cazuri indicau o infec ie, Figura 2.
Patogeneza acestor complica ii precoce cu poten ial
La pacien ii cu necroză infectată se recomadă o
mortal este complexă
(activarea intrapancreatică a
abordare chirurgicală agresivă. Ori de câte ori este
enzimelor digestive, răspunsul in amator sistemic,
posibil, interven ia chirurgicală ar trebui amânată până
stimularea excesivă a celulelor in amatorii, tulburări
în săptămâna a treia sau a patra de evolu ie a bolii, în
microcirculatorii sistemice, stres oxidativ, efect agravant
absen a deteriorării stării clinice [36,38,39]. Majoritatea
al hiperlipidemiei) [13,14,15].
strategiilor chirugicale includ necrectomia, debridarea
Producerea şi eliberarea de enzime diverse, peptide
cu rezec ie segmentară, sechestrectomie, drenaj, lavaj şi
vasoactive, mediatori in amatori, sunt responsabile
retroperitoneostomie. Aceste proceduri în clinici
pentru dezvoltarea şi severitatea disfunc iilor
specializate reduc rata mortalită ii, care în trecut era de
cardiovasculare, pulmonare sau renale [16,17,18].
la 40% la 80%, la o medie de 10% din cazuri [40,41,42].
Complica iile pulmonare cu in ltrate pulmonare
Abcesul pancreatic prezent la aproximativ 3% din
detectabile şi/sau efuziuni pleurale se manifestă la 15%
cazuri, apare în evolu ia pancreatitei severe, de obicei la
până la 55% din pacien ii suferind de pancreatită acută
3-4 săptămâni după debutul pancreatitei acute în
[19,20,21], iar insu cien a respiratorie profundă cu
prezen a colec iilor lichidiene peripancreatice [43,44].
sindrom ARDS la 20% din aceste cazuri [21].
Ar trebui suspectat un abces pancreatic prin intermediul
Complica iile renale cu oligurie pot evolua spre
CT atunci când se observă colec ii lichidiene de mărimi
insu cien ă renală acută, care are o rată a mortalită ii de
diferite la pacien ii cu septicemie având antecedente
80% [22,23].
recente de pancreatită (3-4 săptămâni), lucru demonstrat
Hemoragia
severă
intraabdominală
sau
în studiul nostru în Figura 3, con rmat şi de studiul lui
gastrointestinală
reprezintă
complica ii precoce
Banks [45].
neobişnuite. Alte complica ii hemoragice au loc la 2,5%
Eşecul resorb iei secre iilor pancreatice extravazate
dintre pacien ii cu un prognostic sumbru [24,25].
şi prezen a unui tract de comunicare cu sistemul
În pancreatita acută, hipocalcemia cu valori ale
pancreatic ductal, explică evolu ia nefastă (Figura 4,5).
calciului seric de sub 8mg/dL reprezintă un indicator
În studiul nostru majoritatea pseudochisturilor sunt
prognostic al severită ii bolii [26,27]. Nivelurile calciului
asociate cu locul necrozei, parenchimal, unde se şi
sub 7 mg/dL prevestesc rate mari ale mortalită ii la
dezvoltă, lucru demonstrat în imaginile CT
(Figura
pacien ii cu pancreatită acută.
1,4,5).
Detectarea complica iilor sistemice precoce ale
Drenajul chirugical sau percutan este rezervat
lotului de pacien i studiat (Tabel II) au dus la op iunile
pentru chisturi mai mari de 5 cm şi mai vechi de 6
de tratament adecvat.
săptămâni, chisturi simptomatice
(durere, masă
Cea mai frecventă indica ie pentru interven ie
abdominală, obstruc ia căii gastrice, infec ie sau
chirurgicală în pancreatita acută severă este necroza
hemoragie) [46]. Prezen a pseudochistului hemoragic a
pancreatică infectată. Aceasta este un factor de risc
fost de 18% la o serie de 103 chisturi [47], 12% într-un
pentru sindromul de compartiment abdominal datorat
alt raport cu 132 de chisturi [43] şi de la 2 la 31% în alte
edemului visceral şi retroperitoneal [26,27,28]. Eşecul
studii [37,43,48].
abordării nechirurgicale cere decompresie abdominală.
Ac iunea proteolitică a secre iilor pancreatice
Această complica ie este asociată cu o rată ridicată a
extravazate explică complica iile gastrointestinale şi
MSOF şi a decesului [29,30,31].
biliare în pancreatita acută, iar majoritatea patologiei
Necroza pancreatică apare mai târziu în evolu ie, cel
implică stomacul, duodenul şi colonul transvers, (Figura
mai adesea în săptămâna a treia şi a patra a bolii [32,33].
1), asemănător studiului lui Aly şi colab. în anul 2002
În studiul nostru, necroza infectată a fost detectată
[49].
în primele 2 săptămâni de boală la 19% din pacien i.
Complica iile vasculare nu sunt frecvente în evolu ia
Diagnosticul de necroză pancreatică infectată se pune cu
pancreatitei acute, dar ele pot avea drept rezultat o rată
ajutorul CT, care arată aer sau colec ii retroperitoneale
ridicată a mortalită ii. Dacă nu sunt depistate precoce
84
Sârbu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
pot evolua, generând un pseudoanevrism şi/sau
10.
Matull WR, Pereira SP, O’Donohue JW. Biochemical
hemoragie masivă [50,51].
markers of acute pancreatitis. J Clin Pathol
Majoritatea
complica iilor
hemoragice sau
2006;59(4):340-4.
secundare unui pseudoanevrism care sângerează au o
11.
Liu TH, Kwong KL, Tamm EP, Gill BS, Brown SD,
inciden ă de 10% [52]. Hemoragia intraabdominală
Mercer DW. Acute pancreatitis in intensive care unit
este uşor de identi cat prin imagistică CT [41].
patients: value of clinical and radiologic prognosticators
Inciden a ascitei tranzitorii este observată pe
at predicting clinical course and outcome. Crit Care
imaginea CT relativ frecvent, dar ascita pancreatică
Med 2003;31(4):1026-30.
masivă are o inciden ă foarte scăzută [53].
12.
Buter A, Imrie CW, Carter CR, Evans S, McKay CJ.
Dynamic nature of early organ dysfunction determines
Concluzii
outcome in acute pancreatitis. Br J Surg 2002;89(3):298-
302.
Mortalitatea în pancreatita acută depinde de
13.
Johnson CD, Abu-Hilal M. Persistent organ failure
complica iile poten ial mortale care pot exista şi pot
during the rst week as a marker of fatal outcome in
apare în orice moment al evolu iei pancreatitei. Pot
acute pancreatitis. Gut 2004;53(9):1340-4.
împăr ite în: complica ii precoce care se manifestă în
14.
Brown A, Orav J, Banks PA. Hemoconcentration is an
decursul primelor 2-3 zile; complica ii intermediare în
early marker for organ failure and necrotizing
timpul celei de-a doua până în săptămâna a cincea şi
pancreatitis. Pancreas 2000;20(4):367-72.
complica ii tardive care se manifestă în luni-ani după
15.
Papachristou GI, Whitcomb DC. In ammatory
terminarea unui episod de pancreatită acută.
markers of disease severity in acute pancreatitis. Clin
Depistarea precoce prin metode clinice, imagistice
Lab Med 2005;25(1):17-37.
duce la op iuni de tratament speci ce.
16.
Mayer J, Rau B, Gansauge F, Beger HG. In ammatory
mediators in human acute pancreatitis: clinical and
pathophysiological implications. Gut 2000;47(4):546-
Referințe
52.
17.
Malfertheiner P, Domínguez-Muñoz JE. Prognostic
1.
Halonen KI, Pettilä V, Leppäniemi AK, Kemppainen
factors in acute pancreatitis. Int J Pancreatol
EA, Puolakkainen PA, Haapiainen RK. Multiple
1993;14(1):1-8.
organ dysfunction associated with severe acute
18.
Banks PA, Martin L, Freeman L, et al. Practice
pancreatitis. Crit Care Med 2002;30(6):1274-9.
Guidelines in Acute Pancreatitis. Am J Gastroenterol
2.
Balthazar EJ, Robinson DL, Megibow AJ, Ranson
2006;101(10):2379-400.
JH. Acute pancreatitis: value of CT in establishing
19.
Talamini G, Bassi C, Falconi M, et al. Risk of death
prognosis. Radiology 1990;174(2):331-6.
from acute pancreatitis. Int J Pancreatol 1996;19(1):15-
3.
Buggy BP, Nostrant TT. Lethal pancreatitis. Am J
24.
Gastroenterol 1983;78(12):810-4.
20.
Vriens PW, van de Linde P, Slotema ET, Warmerdam
4.
McKay CJ, Evans S, Sinclair M, Carter CR, Imrie
PE, Breslau PJ. Computed tomography severity index is
CW. High early mortality rate from acute pancreatitis in
an early prognostic tool for acute pancreatitis. J Am Coll
Scotland, 1984-1995. Br J Surg 1999;86(10):1302-5.
Surg 2005;201(4):497-502.
5.
Denham W, Norman J. e potential role of therapeutic
21.
Pastor CM, Matthay MA, Frossard JL. Pancreatitis-
cytokine manipulation in acute pancreatitis. Surg Clin
associated acute lung injury: new insights. Chest
North Am 1999;79(4):767-81.
2003;124(6):2341-51.
6.
Connor S, Alexakis N, Raraty MG, et al. Early and
22.
Buter A, Imrie CW, Carter CR, Evans S, McKay CJ.
late complications after pancreatic necrosectomy. Surgery
Dynamic nature of early organ dysfunction determines
2005;137(5):499-505.
outcome in acute pancreatitis. Br J Surg 2002;89(3):298-
7.
Beger HG, Rau B, Mayer J, Pralle U. Natural course of
302.
acute pancreatitis. World J Surg 1997;21(2):130-5.
23.
Lin HY, Lai JI, Lai YC, Lin PC, Tang GJ. Acute renal
8.
Lowham A, Lavelle J, Leese T. Mortality from acute
failure in severe pancreatitis: A population-based study.
pancreatitis. Int J Pancreatol 1999;25(2):103-6.
Ups J Med Sci 2011;116(2):155-9.
9.
Rocha FG, Benoit E, Zinner MJ, et al. Impact of
24.
Gadacz TR, Trunkey D, Kie er RF Jr. Visceral vessel
radiologic intervention on mortality in necrotizing
erosion associated with pancreatitis. Case reports and a
pancreatitis: the role of organ failure. Arch Surg
review of the literature. Arch Surg 1978;113:1438-
2009;144(3):261-5.
40.
Clinical and Tomographic Aspects of Acute Pancreatitis Complications
85
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
25.
Whitcomb DC. Acute Pancreatitis. N Engl J Med
40.
Bradley EL 3rd. A clinically based classi cation system
2006 18;354(20):2142-50.
for acute pancreatitis. Summary of the International
26.
McMahon MJ, Woodhead JS, Hayward RD. e
Symposium on Acute Pancreatitis, Atlanta, Ga,
nature of hypocalcaemia in acute pancreatitis. Br J Surg
September
11 through
13,
1992. Arch Surg
1978;65(3):216-8.
1993;128(5):586-90.
27.
Nathens AB, Curtis JR, Beale RJ, et al. Management
41.
Singla A, Csikesz NG, Simons JP, et al. National
of the critically ill patient with severe acute pancreatitis.
hospital volume in acute pancreatitis: analysis of the
Crit Care Med 2004;32(12):2524-36.
Nationwide Inpatient Sample
1998-2006. HPB
28.
Büchler MW, Gloor B, Müller CA, Friess H, Seiler
(Oxford) 2009;11(5):391-7.
CA, Uhl W. Acute necrotizing pancreatitis: treatment
42.
Papachristou GI, Takahashi N, Chahal P, Sarr MG,
strategy according to the status of infection. Ann Surg.
Baron TH. Peroral endoscopic drainage/debridement of
2000; 232(5):619-26.
walled-o
pancreatic
necrosis.
Ann Surg
29.
Ashley SW, Perez A, Pierce EA, et al. Necroziting
2007;245(6):943-51.
pancreatitis. Ann Surg 2001;234(4):572-80.
43.
Crass RA, Way LW. Acute and chronic pancreatic
30.
Hungness ES, Robb BW, Seeskin C, Hasselgren PO,
pseudocysts are di erent. Am J Surg 1981;142(6):660-
Luchette FA. Early debridement for necrotizing
3.
pancreatitis: is it worthwhile? J Am Coll Surg
44.
Bucher P, Pugin F, Morel P. Minimally invasive
2002;194(6):740-4.
necrosectomy for infected necrotizing pancreatitis.
31.
Bakker OJ, van Santvoort HC, Besselink MG, van der
Pancreas 2008;36(2):113-9.
Harst E, Hofker HS, Gooszen HG; Dutch Pancreatitis
45.
Banks PA. Acute pancreatitis: medical and surgical
Study Group. Prevention, detection, and management of
management. Am J Gastroenterol
1994;89(8
infected necrosis in severe acute pancreatitis. Curr
Suppl):S78-85.
Gastroenterol Rep 2009;11(2):104-10.
46.
Whitcomb DC. Clinical practice. Acute pancreatitis. N
32.
Werner J, Feuerbach S, Uhl W, Büchler MW.
Engl J Med 2006;354(20):2142-50.
Management of acute pancreatitis: from surgery to
47.
Kiviluoto T, Kivisaari L, Kivilaakso E, Lempinen M.
interventional intensive care. Gut 2005;54(3):426-36.
Pseudocysts in chronic pancreatitis. Surgical results in
33.
De Waele JJ, Hoste E, Blot SI, Decruyenaere J,
102 consecutive patients. Arch Surg 1989;124(2):240-
Colardyn F. Intra-abdominal hypertension in patients
3.
with severe acute pancreatitis. Critical Care
48.
Triester SL, Kowdley KV. Prognostic factors in acute
2005;9(4):452-7.
pancreatitis. J Clin Gastroenterol 2002;34(2):167-76.
34.
Besselink MG, Verwer TJ, Schoenmaeckers EJ et al.
49.
Aly EA, Milne R, Johnson CD. Non-compliance with
Timing of surgical intervention in necrotizing
national guidelines in the management of acute
pancreatitis. Arch Surg 2007;142(12):1194-201.
pancreatitis in the United kingdom. Dig Surg
35.
Hartwig W, Maksan SM, Foitzik T, Schmidt J,
2002;19(3):192-8.
Herfarth C, Klar E. Reduction in mortality with
50.
Cornu-Labat G, Kasirajan K, Simon R, Smith DJ,
delayed surgical therapy of severe pancreatitis. J
Herman ML, Rubin JR. Acute mesenteric vein
Gastrointest Surg 2002;6(3):481-7.
thrombosis and pancreatitis. A rare association. Int J
36.
Besselink MG, van Santvoort HC, Witteman BJ,
Pancreatol 1997;21(3):249-51.
Gooszen HG; Dutch Acute Pancreatitis Study Group.
51.
Burke JW, Erickson SJ, Kellum CD, Tegtmeyer CJ,
Management of severe acute pancreatitis: it’s all about
Williamson BR, Hansen MF. Pseudoaneurysms
timing. Curr Opin Crit Care 2007;13(2):200-6.
complicating pancreatitis: detection by CT. Radiology
37.
Kelly SB, Gauhar T, Pollard R. Massive intraperitoneal
1986;161(2):447-50.
hemorrhage from a pancreatic pseudocyst. Am J
52.
White AF, Baum S, Buranasiri S. Aneurysms secondary
Gastroenterol 1999;94(12):3638-41.
to
pancreatitis.
AJR Am J Roentgenol
38.
Bassi C. Infected pancreatic necrosis. Int J Pancreatol
1976;127(3):393-6.
1994;16(1):1-10.
53.
Johst P, Tsiotos GG, Sarr MG. Pancreatic ascites: a rare
39.
Uhl W, Warshaw A, Imrie C, et al. IAP Guidelines for
complication of necrotizing pancreatitis. A case report
the Surgical Management of Acute Pancreatitis.
and review of the literature. Int J Pancreatol
Pancreatology 2002;2(6):565-73.
1997;22(2):151-4.
86
Sârbu et al
ORIGINAL ARTICLES
TRATAMENTUL NOCTURIEI LA UN GRUP DE PACIENȚI DE SEX
MASCULIN AVÂND SIMPTOMATOLOGIE DE TRACT URINAR INFERIOR
LUTS . REZULTATE PE TERMEN SCURT
Vasile Dan Stanca, Andrei Boc, Radu Aurel Maxim, Vitalie Gherman, Sergiu Nicolescu, Ioan Coman
Departamentul de Urologie, Spitalul Clinic Municipal Cluj-Napoca România
Adresa pentru coresponden ă:
Vasile Dan Stanca
Departamentul Urologie, Spitalul Clinic Municipal Cluj-Napoca,
strada Tăbăcarilor 11, 400139, Cluj-Napoca
Telefon +40.744.622.933, Fax +40.264.485.295
E-mail: vasilestanca@yahoo.com
Primit: 01.02.2014
Acceptat: 20.02.2014
Med Con March 2014, Vol 9, No 1, 87-90
Rezumat
mic ională și frecven ă crescută a mic iunilor. To i
pacien ii cu poliurie nocturnă au înregistrat o reducere a
Nocturia este o problemă majoră a bărba ilor
numărului mic iunilor nocturne; 4 pacien i din cei 6 cu
suferind de simptomatologie de tract urinar inferior
polakiurie nocturnă iritativă au prezentat, de asemenea,
(LUTS). Aproximativ o treime dintre pacien ii cu LUTS
răspuns pozitiv la terapie. Nu am înregistrat niciun efect
prezintă nocturie. Etiologia acestei patologii este încă
secundar cardio-vascular sau urologic.
neclari cată, ind dezbătute multiple teorii cu privire la
Concluzii: Rezultatele noastre sugerează că
mecanismul ziopatologic. Am evaluat rezultatele
tratamentul cu desmopresin 60/120 micrograme/zi este
tratamentului în cazul pacien ilor care prezentau acest
e cient în cazul pacien ilor cu nocturie secundară poliuriei
simptom.
nocturne. Tratamentul cu desmopesin este bine tolerat.
Material și metodă: Am evaluat 29 de bărba i cu
Identi carea mecanismului ziopatologic al nocturiei este
vârsta mai mare sau egală cu 50 de ani. Principala lor
esen ial pentru stabilirea unui tratament e cient.
nemul umire era necesitatea de a se trezi noaptea pentru
Cuvinte cheie: nocturie, simptomatologie de tract
a urina (ca simptom unic sau în asociere cu LUTS).
urinar inferior, desmopresin, alfa-blocan i, antimuscarinice
Bilan ul diagnostic standard a inclus completarea unui
jurnal mic ional. Pacien ii cu nocturie secundară
Introducere
poliuriei nocturne au urmat tratament cu desmopresin
60 sau 120 micrograme/zi, timp de 30 de zile; pacien ii
Nocturia este de nită de către Societatea
cu mic iuni nocturne în cantitate mică au fost trata i cu
Interna ională a Continen ei ca disconfortul individului
alfa blocan i și antimuscarinic. Am evaluat rezultatele și
de a se trezi noaptea o dată sau de mai multe ori pentru
efectele secundare ale acestui tratament.
a mic iona și reprezintă un simptom comun, cu un
Rezultate: Din numărul total de pacien i care
impact semni cativ asupra calită ii somnului și calită ii
prezentau jenă rela ionată cu urinarea nocturnă, 79,3%
vie ii
[1]. Este o patologie cu prevalen ă mare, care
(23 de pacien i) au prezentat nocturie secundară
totuși este subdiagnosticată [2].
poliuriei nocturne (1-5 urinări/noapte); 6 pacien i au
Tradi ional a fost considerată ca o patologie asociată
prezentat nocturie iritativă asociată cu urgen ă
hiperplaziei benigne de prostată și a primit un tratament
Treatment of Nocturia in a Male Group of Patients With Lower Urinary Tract Symptoms (LUTS). Short-Term Results
87
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
adresat prostatei. Punctul
7 din Chestionarul
asupra tratamentului ind dictată de ziopatologia
Interna ional al Simptomelor Prostatei (International
mic iunilor nocturne.
Prostatic Symptoms Score; IPSS) se adresează problemei
urinatului nocturn („În ultima lună, de câte ori a trebui
Material şi metode
să vă trezi i să urina i, din momentul în care v-a i culcat și
până în momentul în care v-a i trezit diminea a”?). În
Am inclus în studiu bărba i cu vârsta de 50 de ani
ultimul deceniu, ziopatologia nocturiei a fost mai bine
sau mai mult, care se plâng de necesitatea de a se trezi
în eleasă și au început să e incrimina i și al i factori, nu
noaptea pentru a urina, simptom unic sau asociat cu
doar prostata. Poliuria nocturnă, sindromul vezicii
LUTS. Am exclus din studiu pacien ii cu patologii care
hiperactive sau patologiile non-urologice, cum ar
necesitau tratament speci c: infec ii de tract urinar,
hipertensiunea arterială sau insu cien a cardiacă
malignită i cunoscute sau suspectate, obstruc ie
congestivă au fost studiate ca factori etiologici [3].
subvezicală semni cativă, cu reziduu postmic ional mai
Această abordare complexă a patogenezei nocturiei
mare de 100 ml și func ie vezicală redusă și pacien ii
a fost declanșată de diverse observa ii. În primul rând,
care prezentau comorbidită i care pot interfera cu
prevalen a este asemănătoare în rândul femeilor și al
administrarea de antimuscarinic, alfablocant sau
bărba ilor. Într-un studiu
nlandez, prevalen a
desmopresină (glaucom sau hiponatremie).
standardizată pe vârstă a nocturiei (una sau mai multe
Bilan ul diagnostic standard a inclus anamneza,
mic iuni per noapte) a fost de aproximativ
40% la
examenul obiectiv, măsurarea ecogra că a reziduului
ambele sexe. A fost sensibil mai frecvent întâlnită în
postmic ional și jurnal mic ional. Cel din urmă a fost
cazul femeilor tinere decât în cazul bărba ilor; în grupul
un test pivotal care ne-a permis să de nim două grupe
de vârstă 50-59 ani inciden a a fost egală, jumătate
de pacien i: pacien i cu nocturie datorită poliuriei
dintre femei și bărba i prezentând nocturie, pe când
nocturne sau cu o diureză nocturnă mai mare de 400 ml
după 60 de ani, bărba ii au fost semni cativ mai afecta i
și pacien i cu volum mic ional mic.
[4]. Acest tipar de evolu ie sugerează atât prezen a altor
Pacien ii din primul grup au fost trata i cu
etiologii non-prostatice, cât și a etiologiilor prostatice
desmopresin 60 micrograme/zi (dacă aveau vârsta mai
ale bărbatului care îmbătrânește.
mare de 65 ani) sau 120 micrograme/zi (vârsta sub 65
Sindromul vezicii hiperactive este altă patologie care
ani) pentru 30 de zile; pacien ii cu volume mic ionale
poate duce la mic iuni nocturne. Societatea
nocturne mici au fost trata i cu o asociere
Interna ională a Continen ei (ICS) de nește sindromul
medicamentoasă dintre un alfa blocant și un
vezicii hiperactive (OAB) ca o asociere de simptome,
antimuscarinic. Am monitorizat nivelul seric al sodiului
incluzând urgen a mic ională asociată cu frecven ă
pentru to i pacien ii trata i cu desmopresin, după 7 zile
crescută și nocturie
[5]. Tipic, se întâlnesc mic iuni
de tratament.
nocturne de cantită i mici. Această patologie este foarte
Finalul studiului a fost reducerea numărului de
frecvent întâlnită la pacien i cu OAB, aproximativ 75%
mic iuni nocturne cu minim un episod/noapte. În acest
dintre ei raportând unul sau mai multe episoade de
sens, am încercat să tratăm pacien ii în func ie de
nocturie per noapte [6].
mecanismul ziopatologic suspectat și nu în func ie de
Multiple patologii non-urologice au fost incriminate
etiologie.
recent în etiologia mic iunilor nocturne. Studiile
Am evaluat rezultatele și efectele secundare ale
epidemiologice raportează o legătură semni cativă între
acestui tratament; pacien ii au fost reevalua i urmând
nocturie și patologii precum hipertensiunea arterială sau
același protocol, după 30 de zile.
disfunc iile respiratorii pe timpul nop ii. Rela ia cauză-
efect dintre ele încă nu a fost dovedită, dar efectele
Rezultate
hipertensiunii arteriale asupra ltrării glomerurale și
transportul tubular, eliberarea de peptid natriuretic
Am evaluat un număr de 29 bărba i cu vârsta
atrial și edemul periferic pot juca un rol important în
cuprinsă între 53 și 84 ani care prezentau nocturie, în
apari ia mic iunilor nocturne [7,8].
cadrul serviciului nostru, între ianuarie 2011 și aprilie
Deoarece patologia este multifactorială, decizia
2012.
asupra unui tratament trebuie să ia în calcul to i
Din numărul total de pacien i cu episoade
poten ialii factori etiologici. Luând în calcul to i acești
deranjante de mic iuni nocturne 79,3% (23 pacien i) au
factori, am decis să evaluăm rezultatele tratamentului
avut nocturie secundară diurezei nocturne crescute
medicamentos în cazul pacien ilor care se plâng de
(peste 400 ml/noapte). Diureza nocturnă pentru acest
nocturie (ca simptom unic sau asociat cu LUTS), decizia
grup de pacien i a fost cuprinsă între 400-1200 ml.
88
Stanca et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Zece dintre acești pacien i aveau vârsta mai mare de 65
Pentru pacien ii cu nocturie și cantită i crescute ale
ani și au primit 60 micrograme desmopresin/zi; ceilal i
urinii emise noaptea (considerăm 400 ml urină/noapte
13 pacien i au primit o doză zilnică de 120 micrograme
un prag acceptabil) doar tratamentul antidiuretic
desmopresin. To i acești pacien i au înregistrat o scădere,
(desmopresin) oferă șansa unei ameliorări semni cative
cu minim un episod, a numărului de mic iuni per
a simptomatologiei [13]. Acest rol al moleculei a fost
noapte, după 30 zile de tratament cu desmopresin.
studiat în ultimii 10 ani, iar pro lul ei de siguran ă a
Șase pacien i
(20,7%) au prezentat mic iuni cu
fost stabilit [14]. Principala limitare a utilizării sale este
volum scăzut, asociate cu urgen ă mic ională sau
riscul de hiponatremie, care ar putea
mai mare la
frecven ă crescută. Patru dintre acești 6 pacien i au avut
pacien ii peste 65 ani. Multiple studii recente atenuează
rezultate pozitive în urma tratamentului, reducându-se
aceste neliniști: femeile prezintă un risc mai mare decât
mic iunile nocturne cu minim un episod/noapte.
bărba ii de orice vârstă, iar o doză de 60 micrograme/zi
Ceilal i doi pacien i au declarat că simptomele lor au
poate prescrisă bărba ilor de orice vârstă, fără a crește
fost nemodi cate.
riscul de diselectrolitemie [15]. În studiul nostru am
Nu am înregistrat niciun efect secundar cardio-
folosit doze de 60 micrograme desmopresină/zi pentru
vascular sau urologic. Nivelul seric al sodiului a fost mai
bărba i cu vârsta peste 65 ani și nu am înregistrat cazuri
mare de 130 mmol/l pentru to i pacien ii, după 7 zile de
de hiponatremie, sau alte efecte secundare.
tratament.
Când capacitatea de stocare a vezicii pare afectată,
terapia combinată cu alfa-blocant și antimuscarinic
Discuții
oferă cele mai bune rezultate
[16]. Majoritatea
pacien ilor noștri care apar in acestui grup, au înregistrat
Tratamentul nocturiei a reprezentat mereu o
îmbunătă irea simptomatologiei după
30 de zile de
provocare pentru urologi. Conceptele timpurii de
tratament.
tratament includeau mic iunile nocturne în mijlocul
simptomelor cauzate de obstruc ia subvezicală. Astfel, o
Concluzii
reducere a numărului de mic iuni nocturne era așteptată
în urma tratamentului intit pe hiperplazia benignă de
Majoritatea pacien ilor au avut nocturie secundară
prostată. Tratamentul cu alfa-blocaan i a avut rezultate
produc iei nocturne crescute de urină. Rezultatele
dezamăgitoare: reducerea netă a mic iunilor vezicale a
noastre sugerează că tratamentul cu desmopresin 60/120
fost cu 0,3 per noapte fa ă de placebo pentru terazosin
micrograme/zi este e cient în cazul pacien ilor cu
sau terazosin cu nasteridă într-un studiu publicat în
nocturie secundară produc iei nocturne crescute de
2003 [9] și rezultatele au fost con rmate și de alte studii
urină. Tratamentul cu desmopresin a fost bine tolerat.
[10].
Alfa-blocantul și antimuscarinicul ar trebui administrate
Când vezica urinară a fost învinuită pentru această
doar pacien ilor care se plâng de urgen ă mic ională și
patologie, antimuscarinicele au fost prescrise tuturor
frecven ă
mic ională
crescută.
Identi carea
pacien ilor cu nocturie. Rezultatele au fost la fel de
mecanismului ziopatologic al nocturiei este esen ial
dezamăgitoare, bene ciul net asupra placebo a constat
pentru stabilirea unui tratament e cient. Părerea noastră
într-o reducere a numărului de mic iuni nocturne cu
este că în cazul bărba ilor cu nocturie decizia terapeutică
0,05-0,29 pentru diferite molecule
(solifenacin,
ar trebui ghidată de mecanismul ziopatologic și nu de
trospium, etc) [11,12].
considera iile anatomice sau etiologice.
Patologia este multifactorială și mul i factori
etiologici sunt necunoscu i sau inaccesibil terapiei.
Conflicte de interese
Printre aceștia este și eliberarea defectuoasă de peptid
natriuretic atrial. Considerăm că singura modalitate
Autorii nu au nimic de declarat.
posibilă de abordare a nocturiei este de a identi ca
mecanismul de ac iune: diureză nocturnă crescută (peste
capacitatea func ională a vezicii), vezică hiperactivă
Referințe
(mic iuni cu volum scăzut), sau urină reziduală care
reduce capacitatea de stocare a urinii. Cea din urmă
1. van Kerrebroeck P, Abrams P, Chaikin D, et al. e
situa ie poate
ușor identi cată prin ecogra e
standardization of terminology in nocturia: report from
abdominală și are tratament speci c, dar pentru primele
the Standardization Sub-committee of the International
două situa ii gra cele frecven ă-volum sunt instrumente
Continence
Society.
Neurourol
Urodyn
indispensabile pentru selec ia tratamentului.
2002;21(2):179-83.
Treatment of Nocturia in a Male Group of Patients With Lower Urinary Tract Symptoms (LUTS). Short-Term Results
89
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
2.
van Doorn B, Bosch JL. Nocturia in older men.
secondary analysis of the Department of Veterans A airs
Maturitas 2012;71(1):8-12.
Cooperative Study Trial. J Urol 2003;170(1):145-8.
3.
Cornu JN, Abrams P, Chapple CR et al. A
10.
Park HK, Kim HG. Current evaluation and treatment
contemporary assessment of nocturia: de nition,
of nocturia. Korean J Urol 2013;54(8):492-8.
epidemiology, pathophysiology, and management--a
11.
Brubaker L, FitzGerald MP. Nocturnal polyuria and
systematic review and meta-analysis. Eur Urol
nocturia relief in patients treated with solifenacin for
2012;62(5):877-90.
overactive bladder symptoms. Int Urogynecol J Pelvic
4.
Tikkinen KA, Tammela TL, Huhtala H, Auvinen A.
Floor Dysfunct 2007;18(7):737-41.
Is nocturia equally common among men and women? A
12.
Rudy D, Cline K, Harris R, Goldberg K, Dmochowski
population based study in Finland. J Urol
R. Multicenter phase III trial studying trospium chloride
2006;175(2):596-600.
in patients with overactive bladder. Urology
5.
Natalin R, Lorenzetti F, Dambros M. Management of
2006;67(2):275-80.
OAB in ose Over Age
65. Curr Urol Rep
13.
van Kerrebroeck P, Rezapour M, Cortesse A, üro
2013;14(5):379-85.
J, Riis A, Nørgaard JP. Desmopressin in the treatment of
6.
Irwin DE, Abrams P, Milsom I, Kopp Z, Reilly K.
nocturia: a double-blind, placebo-controlled study. Eur
EPIC Study Group. Understanding the elements of
Urol 2007;52(1):221-9.
overactive bladder: questions raised by the EPIC study.
14.
Mattiasson A, Abrams P, Van Kerrebroeck P, Walter S,
BJU Int 2008;101(11):1381-7.
Weiss J. E cacy of desmopressin in the treatment of
7.
Feldstein CA. Nocturia in arterial hypertension: a
nocturia: a double-blind placebo-controlled study in
prevalent, underreported, and sometimes underestimated
men. BJU Int 2002;89(9):855-62.
association. J Am Soc Hypertens 2013;7(1):75-84.
15.
Juul KV, Klein BM, Sandström R, Erichsen L, Nørgaard
8.
Parthasarathy S, Fitzgerald M, Goodwin JL, Unruh
JP. Gender di erence in antidiuretic response to desmopressin.
M, Guerra S, Quan SF. Nocturia, sleep-disordered
Am J Physiol Renal Physiol 2011;300(5):F1116-22.
breathing, and cardiovascular morbidity in a
16.
Van Kerrebroeck P, Haab F, Angulo JC, et al. E cacy
community-based cohort. PLoS One 2012;7(2):e30969.
and safety of solifenacin plus tamsulosin OCAS in men
9.
Johnson TM 2nd, Jones K, Williford WO, Kutner
with voiding and storage lower urinary tract symptoms:
MH, Issa MM, Lepor H. Changes in nocturia from
results from a phase 2, dose- nding study (SATURN).
medical treatment of benign prostatic hyperplasia:
Eur Urol 2013;64(3):398-407.
90
Stanca et al
ORIGINAL ARTICLES
ANALIZĂ CU ELEMENT FINIT A UNEI NOI CUŞTI EXPANDABILE
PENTRU FUZIUNE INTERVERTEBRALĂ
Mihai Magureanu1, Dinu Vermesan2, Juganaru Iulius2, Horia Haragus2, Roberta Cecilia Avram4,
Dan Ioan Stoia3, Gigi Adrian Aiordachioaie4
1Compartimentul de Chirurgie Spinală, Spitalul Colentina, Bucureşti, 2Clinica I Ortopedie-Traumatologie, Universitatea
de Medicină şi Farmacie „Victor Babeş” Timişoara, 3Departamentul de Mecanică şi Vibra ii, Universitatea Politehnică
Timişoara, 4Compartimentul de Fiziologie şi Fiziopatologie Universitatea de Vest „Vasile Goldiş” Arad, 5Clinica II de
Chirurgie, Universitatea de Vest „Vasile Goldiş” Arad
Adresa pentru coresponden ă:
Haragus Horia
Clinica I Ortopedie traumatologie,
Spitalul Clinic Judetean de Urgen ă Timişoara
B-dul Iosif Bulbuca nr 10, 300736, Timişoara, România
Tel +40747025064, Fax +40256487144
E-mail: horia.haragus@yahoo.com
Primit: 01.11.2013
Acceptat: 15.01.2014
Med Con March 2014 Vol 9, No 1, 91-96
Rezumat
au fost semni cativ mai mari cu cușca închisă și lordoza
modi cată. Astfel
această
cușcă
expandabilă
Durerea lombară cronică este cauzată de degenerarea
experimentală ar putea limita stresul asupra discului
segmentelor distale ale coloanei vertebrale. Tendin ele
supraiacent prin restaurarea lordozei ziologice și astfel
actuale se concentrează pe chirurgia minim invazivă.
să prevină progresia bolii și degenerarea discală proximală.
Astfel, ne-am propus să determinăm impactul asupra
Cuvinte cheie: fuziune lombară, fuziune
discului supraiacent a unei cuști expandabile pentru
intervertebrală lombară posterioară
(PLIF), fuziune
fuziune intervertebrală lombară transforaminală (TLIF)
intervertebrală transforaminală (TLIF)
nou dezvoltate folosind modelare prin metoda
elementului nit. Simulările numerice au fost efectuate
Introducere
comparativ pentru două structuri diferite: cușca închisă
și expandată la
12 grade. Aceasta se translatează în
Durerea lombara cronică este cauzată de degenerarea
modelul scheletal prin plăcile terminale L4-L5 paralele și
segmentelor distale ale coloanei vertebrale. Mai mul i
respectiv cu o lordoză de
14,2 grade. To i ceilal i
factori etiopatogenetici sunt cunoscu i, în timp ce unii
parametri au fost păstra i constan i. Pentru ecare
rămân neelucida i. Degenerarea discală este cauza
situa ie am efectuat 12 simulări intite la a reproduce
principală, urmată de artroza articula iilor zigomatice.
diferite grade de exie lombară ziologică. Am de nit
Pe măsură ce discul degenerează poate hernia și astfel
unghiurile de rota ie pentru vertebra L3 și am păstrat
cauza compresii focale. Pe măsură ce boala progresează
segmentul L4-L5 fuzionat rigid. Efectele au fost măsurate
discul colabează, iar foramenurile și canalul spinal
în deformarea elastică și deplasarea unui model discal
vertebral se îngustează. Articula iile zigomatice pot o
L3-L4. Pentru toate simulările deformarea și deplasarea
sursă de durere în sine. Pe măsură ce acestea degenerează,
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
91
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
segmentul proximal poate aluneca anterior și duce la
pentru PLIF, cât și pentru TLIF: leziuni neurologice
stenoză a canalului vertebral, o situa ie numită
intraoperatorii iatrogene, migrarea sau înfundarea
spondilolisteză. Procesul in amator rezultant poate
implantului, leziuni ale sacului dural, infec ii, osi cări
limitat la esuturile musculoscheletale, sau poate avansa
heterotopice, radiculită legată de proteine morfogenetice
la măduvă și emergen ele
(rădăcinile) nervoase, cu
osoase (BMP) și osteoliză [4].
de cit neurologic asociat - radiculopatie. Alte cauze de
Astfel, ne-am propus să determinăm impactul
durere lombară joasă pot prezenta simptome similare,
asupra discului supraiacent a unei cuști expandabile
dar care nu sunt legate de degenerări structurale primare:
pentru fuziune intervertebrală lombară transforaminală
tumori, infec ii, deformări, sechele posttraumatice,
(TLIF) nou dezvoltate, folosind modelare prin metoda
osteoporoză, boli autoimune, întinderi musculare,
elementului nit.
obezitate morbidă și sarcină. Cu toate că artrodeza
spinală nu e un concept nou, fuziunea intervertebrală
Material şi metodă
posterioară
(PLIF) a fost introdusă de Clowart și a
reprezentat o evolu ie semni cativă în tratamentul
Analiza prin metoda elementului nit este o
operator al tulburărilor spinale [1].
procedură numerică folosită pe larg pentru a ob ine solu ii
Tendin ele actuale se concentrează pe chirurgia
la ecua ii complexe care descriu sau aproximează o
minim invazivă. Această abordare este determinată mai
mul ime de fenomene zice. Fundamentul acestei metode
mult de afectări musculare și ligamentare limitate decât
constă în conceptul că un domeniu complex poate
de incizii mici ale pielii. Fuziunea intervertebrală
subdivizat într-o serie de regiuni mai mici de nite prin
lombară transforaminală minim invazivă (MIS-TLIF)
ecua ii diferen iale calculabile, proces denumit discretizare.
ca metodă de a ob ine fuziune circumferen ială folosind
Asamblarea ulterioară a acestor seturi de ecua ii duce la
un abord posterior unilateral și retractoare tubulare
determinarea întregului domeniu. În studiul nostru am
inserate prin dilatări musculare a dus deja la raportarea
folosit programul ANSYS Workbench 13.
de rezultate favorabile pentru durere lombară joasă și
radiculopatie asociată spondilolistezei, degenerării
Tabel I. Proprietă ile mecanice
discale și hernierii discale recurente [2].
ale materialelor folosite la analiză
Au fost propuse ansambluri TLIF cu costuri limitate
Proprietate
Modulul
Coe cien-
Density
și cu rezultate favorabile. Fuziunea intervertebrală
lui Young
tul lui
[kg/mm3]
Material
[MPa] Poisson [-]
lombară
transforaminală
cu
instrumenta ie
Ti-6Al-4V
96000
0,36
4,62*10-6
transpediculară unilaterală și un șurub translaminar
O el inoxidabil austenitic
1,93*105
0,31
7,75*10-6
poate reduce costul implanturilor posterioare cu aproape
Os cortical
1,20*105
0,34
3.21*10-6
50% [3]. Mai multe complica ii au fost descrise atât
Disc intervertebral
250
0,35
-
A
B
Figura 1. Stadiile de discretizare ale modelului de studiu cu cuşca închisă şi expandată;
A - discretizare preliminară, B - ra nări ulterioare şi cuşca deschisă
92
Magureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Am început prin analizarea achizi iilor CT (computer
Simularile numerice au fost efectuate folosind
tomograf ) de la 3 pacien i (1-bărbat de 49 ani, 2-femeie
modulul Workbench Simulation pentru două situa ii:
de 55 ani și 3-bărbat de 47 ani) cu durere lombară joasă și
închis și expandat (lordoza restaurată) (Figura 1).
modi cări degenerative incipiente ale discurilor lombare
intă pentru modelarea noastră (L3, L4, L5). Am construit
Rezultate
astfel un model 3D reprezentativ pentru vertebrele mai
sus men ionate. Acesta a fost apoi importat în programul
Simulările numerice au fost efectuate comparativ
pentru analiză cu element nit și i s-au atribuit proprietă i
pentru două structuri diferite: cușca închisă și expandată
materiale corespunzătoare
(modul de elasticitate
la 12 grade. Aceasta se translatează în modelul scheletal
longitudinal și coe cientul lui Poisson, Tabel I).
prin plăcile terminale L4-L5 paralele și respectiv cu o
A. Deformarea elastică echivalentă
B. Deplasarea totală
C. Deformarea elastică normală
D. Deformarea elastică la forfecare
Figura 2. Rezultatele analizei numerice cu cuşca expandată
E. Deformarea totală
F. Deformarea elastică
Figura 3. Selec ii ale deformării totale (E) şi elastice (F) respectiv, pe o sec iune a discului intervertebral L3
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
93
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Tabel II. Deforma iile elastice comparative şi deplasarea totală în cele 12 simulari cu cuşca închisă şi deschisă
Deformarea elastică [mm/mm]
Deplasarea totală [mm]
Test
Deplasare angulară L3 [grd] la 500 N
Cuşca închisă Cuşca deschisă Cuşca închisă Cuşca deschisă
1
1,0
0,150
0,04
0,950
0,47
2
1,8
0,280
0,14
1,730
0,86
3
2,6
0,411
0,195
2,510
1,43
4
3,4
0,520
0,26
3,110
1,64
5
4,2
0,660
0,301
4,070
2,01
6
5,0
0,790
0,39
4,850
2,42
7
5,8
0,920
0,44
5,630
2,94
8
6,6
1,050
0,52
6,400
3,2
9
7,4
1,900
0,61
7,120
3,67
10
8,2
1,300
0,65
7,970
3,98
11
9,0
1,430
0,69
8,750
4,49
12
9,8
1,590
0,78
9,700
4,76
Medie
0,916
0,418
5.232
2.655
SD
0,550
0,236
2.843
1.412
-
p
0,008
0.010
95% CI
0,139-0,857
0.675-4.477
lordoză de 14,2 grade. To i ceilal i parametrii au fost
discală a segmentului adiacent proximal. Într-un raport al
păstra i constan i. Pentru ecare situa ie am efectuat 12
Registrului Suedez Spinal (SweSpine), stenoza lombară
simulari intite pentru a reproduce diferite grade de
este cea mai frecventă indica ie pentru tratament
exie lombară ziologică. Am de nit unghiurile de
chirurgical. Artroplastia spinală lombară are rezultate
rota ie pentru vertebra L3 și am păstrat segmentul L4-
comparabile cu fuziunea pentru durerea datorată
L5 fuzionat rigid. Efectele au fost măsurate în
degenerarii discale [6]. În cadrul grupului de studiu spinal
deformarea elastică și deplasarea unui model discal L3-
lombar suedez, Fritzell și colab. au efectuat o compara ie
L4. Datele, alături de compara ia prin metoda T-test
prospectivă randomizată a tehnicilor chirurgicale uzuale
(GraphPad) sunt expuse în Tabelul II.
folosite pentru fuziune la pacien ii cu durere lombară
Pentru toate simulările deformarea și deplasarea au
cronică severă. Toate tehnicile au fost egal e ciente în a
fost semni cativ mai mari cu cușca închisă și lordoza
reduce durerea (VAS) și a scădea dizabilitatea (ODI).
modi cată. Astfel
această
cușcă
expandabilă
Fuziunea posterolaterală simplă
(PLF) a avut rate de
experimentală ar putea limita stresul asupra discului
consolidare radiogra că mai scăzute, dar și mai pu ine
supraiacent prin restaurarea lordozei ziologice și astfel
complica ii și costuri reduse comparativ cu procedurile
să prevină progresia bolii și degenerarea discală proximală.
circumferen iale mai complexe (fuziune intervertebrală
anteroposterioară) cu rezultate similare [8].
Discuții
Recenzia ghidului practic clinic al Societă ii
Americane de Studiu al Durerii din
2009 asupra
O recenzie sistematică a bolii lombare degenerative
chirurgiei pentru durerea lombară are rezultate nuan ate
simptomatice la pacien i trata i conservator sau prin
în favoarea ziokinetoterapiei. Astfel pentru durerea
fuziune a identi cat îmbunătă iri mai mari ale ODI
lombară degenerativă non-radiculară, fuziunea este ușor
(indexul de dizabilitate Oswestry) pentru spondilolisteză
spre moderat superioară tratamentului conservator, cu
și boala discală degenerativă, comparativ cu pacien ii cu
mai pu in de jumătate din pacien i având rezultate
durere lombară cronică, indiferent de tehnică [5].
optime. Pentru hernia discală cu radiculopatie există
În plus, la pacien ii cu durere lombară, artroplastia
dovezi care arată că discectomia este superioară
discală și stabilizarea posterioară dinamică după
tratamentului conservator. Pentru stenoza spinală
decompresie oferă rezultate ușor superioare comparativ cu
simptomatică
(cu sau fără spondilolisteză) există de
fuziunea și nu au reușit să atingă îmbunătă irile ob inute
asemenea dovezi bune că decomprimarea chirurgicală
după artroplastia totală a șoldului sau genunchiului [6,7];
este superioară abordării conservatoare. Artroplastia
fuziunea este încă standardul de aur și aceasta procedură
discală are e cien ă similară cu fuziunea pentru boala
poate produce complica ii speci ce cum este degenerarea
discală degenerativă la un nivel, iar spa iatoarele
94
Magureanu et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
interspinoase sunt superioare tratamentului conservator
2.
Holly LT, Schwender JD, Rouben DP, Foley KT.
în stenoza spinală [7].
Minimally invasive transforaminal lumbar interbody
Evaluarea RMN (rezonan a magnetică nucleară) a
fusion: indications, technique, and complications.
degenerărilor discale intervertebrale lombare a aratat că
Neurosurg Focus 2006;20(3):E6.
modi carile Modic corelează cu gradele P rrmann
3.
Sethi A, Lee S, Vaidya R. Transforaminal lumbar
pentru degenerare discală, însă nu există corela ie între
interbody fusion using unilateral pedicle screws and a
gradele Modic și rezultatele după tratament chirurgical
translaminar screw. Eur Spine J 2009;18(3):430-4.
[9]. Rezultate superioare s-au ob inut prin artroplastie
4.
Chrastil J, Patel AA. Complications associated with
discală lombară la pacien i cu modi cari tip Modic 1 ale
posterior and transforaminal lumbar interbody fusion. J
plăcilor terminale pe achizi ii RMN preoperatorii [10].
Am Acad Orthop Surg 2012;20(5):283-91.
Tehnica TLIF nu are complica iile poten iale
5.
Carreon LY, Glassman SD, Howard J. Fusion and
descrise pentru fuziunea intervertebrală lombară
nonsurgical treatment for symptomatic lumbar
combinată anteroposterioară și PLIF în ob inerea unei
degenerative disease: a systematic review of Oswestry
fuziuni circumferen iale. Partea fa etectomiei se alege în
Disability Index and MOS Short Form-36 outcomes.
func ie de simptomele pacientului. În plus, duce la
Spine J 2008;8(5):747-55.
durată operatorie mai scăzută, injurii neurologice mai
6.
Strömqvist B, Fritzell P, Hägg O, Jönsson B, Sandén
pu ine și rezultate de ansamblu mai bune [11]. Totuși
B; Swedish Society of Spinal Surgeons. Swespine: the
pentru spondilolisteza istmică, adaugarea unei fuziuni
Swedish spine register :
e 2012 report. Eur Spine J
intervertebrale conferă rezisten ă mecanică superioară
2013;22(4):953-74.
comparativ cu instrumenta ia posterioară simplă.
7.
Chou R, Baisden J, Carragee EJ, Resnick DK, Sha er
Aceasta ajută la păstrarea corec iei și poate in uen a
WO, Loeser JD. Surgery for low back pain: a review of
rezultatele clinice
[12]. Fuziunea spinală corectă
the evidence for an American Pain Society Clinical
anteroposterioară are rezultate similare cu PLIF în
Practice Guideline. Spine
(Phila Pa
1976)
privin a rezultatelor clince și func ionale, precum și a
2009;34(10):1094-109.
ratelor de fuziune. Complica iie intraoperatorii sunt
8.
Fritzell P, Hägg O, Wessberg P, Nordwall A; Swedish
mai mari în primul grup, în principal datorită lacerărilor
Lumbar Spine Study Group. Chronic low back pain
venoase din abordul retroperitoneal anterior. Pe de altă
and fusion: a comparison of three surgical techniques: a
parte, complica iile postoperatorii pot
mai mari în
prospective multicenter randomized study from the
grupul TLIF datorită extrudărilor de material pentru
Swedish lumbar spine study group. Spine (Phila Pa
grefare la nivelul rădăcinilor nervoase [13]. Într-un alt
1976) 2002;27(11):1131-41.
studiu, ratele de neconsolidare și rezultatele clinice în
9.
Yu LP, Qian WW, Yin GY, Ren YX, Hu ZY. MRI
fuziunea intervertebrală lombară posterioară au fost
assessment of lumbar intervertebral disc degeneration
similare cu TLIF. Totuși restaurarea înăl imii discale și a
with lumbar degenerative disease using the P rrmann
lordozei au fost superioare prin tehnica PLIF, în timp ce
grading systems. PLoS One 2012;7(12):e48074.
pierderea sangvină, timpul operator și costurile au fost
10.
Blondel B, Tropiano P, Gaudart J, Huang RC, Marnay
mai mici cu tehnica TLIF [14].
T. Clinical results of lumbar total disc arthroplasty in
Studiul prin metoda elementului nit a identi cat
accordance with Modic signs, with a 2-year-minimum
încărcări scăzute și postura îmbunătă ită când cușca a
follow-up. Spine (Phila Pa 1976) 2011;36(26):2309-
fost expandată. Acestea pot constitui premizele pentru
15.
rezultate clinice îmbunătă ite, precum și inciden ă
11.
Mura PP, Costaglioli M, Piredda M, Caboni S, Casula
scăzută de degenerare a discului supraiacent după
S. TLIF for symptomatic disc degeneration: a
fuziunea lombară. Cu toate acestea, pentru ecare caz
retrospective study of 100 patients. Eur Spine J 2011;20
trebuie particularizate toate tehnicile de abord și luate în
Suppl 1:S57-60.
considerare stabilizarea posterioară dinamică și
12.
La Rosa G, Conti A, Cacciola F, Cardali S, La Torre
înlocuirile discale.
D, Gambadauro NM, Tomasello F. Pedicle screw
xation for isthmic spondylolisthesis: does posterior
lumbar interbody fusion improve outcome over
Referințe
posterolateral fusion? J Neurosurg
2003;99(2
Suppl):143-50.
1. Cloward RB. e treatment of ruptured intervertebral
13.
Faundez AA, Schwender JD, Safriel Y, Gilbert TJ,
discs by vertebral body fusion. I. Indications, operative
Mehbod AA, Denis F, Transfeldt EE, Wroblewski JM.
technique, after care. J Neurosurg 1953;10:154-68.
Clinical and radiological outcome of anterior-posterior
Finite Element Analysis Of A New Expandable Interbody Fusion Cage
95
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
fusion versus transforaminal lumbar interbody fusion for
14. Jiang SD, Chen JW, Jiang LS. Which procedure is better
symptomatic disc degeneration: a retrospective
for lumbar interbody fusion: anterior lumbar interbody
comparative study of
133 patients. Eur Spine J
fusion or transforaminal lumbar interbody fusion? Arch
2009;18(2):203-11.
Orthop Trauma Surg 2012;132(9):1259-66.
96
Magureanu et al
ORIGINAL ARTICLES
APENDECTOMIA LA OBEZI. ABORD CLASIC SAU LAPAROSCOPIC?
Marius Sfîrlea1, Adrian Maghiar1, Teodor Maghiar2, Dan Ciurtin1, Codru a Macovei1, George Dejeu1,
Ciprian Borza2, Daniela Berdea3, Daniela Rahotă4
1Clinica de Chirurgie Generală, 2Sec ia Urologie, 3Sec ia Radiologie şi Imagistică, 4Departamentul de Igienă, Spitalul
Pelican Oradea, a liat Facultă ii de Medicină şi Farmacie, Universitatea Oradea, România, Clinica Chirurgie 1 a
Spitalului Clinic Jude ean Oradea şi Clinica Chirurgie a Spitalului Clinic Pelican Oradea
Adresa pentru coresponden ă:
Sfîrlea Marius
Spital Pelican, str. Corneliu Coposu nr. 2, Oradea, Bihor
E-mail: s rleamarius@yahoo.com
Primit: 25.08.2013
Acceptat: 28.02.2014
Med Con March 2014, Vol 9, No 1, 97-101
Rezumat
(51 fa ă de
48 minute). Complica iile infec ioase
precoce au fost mai pu in frecvente la lotul prin
Obezii reprezintă o categorie aparte de pacien i care
laparoscopie (22,7% vs. 73,3%). Complica ia majoră a
prezintă comorbidită i mai frecvente și risc anestezic
fost abcesul profund, câte un caz în ecare din cele două
mai mare, comparativ cu pacien ii cu greutate corporală
loturi de pacien i. Necesarul de antialgice postoperator a
normală. Din punct de vedere chirurgical manevrele
fost mai mic (90% vs. 42%) pentru pacien ii opera i
operatorii sunt îngreunate de grosimea peretelui
miniinvaziv. Durata și costurile de spitalizare au fost mai
abdominal și de volumul mare de grăsime peritoneală
mici în lotul pacien ilor opera i miniinvaziv decât în
care acoperă câmpul de lucru. Introducerea tehnicilor
lotul celor opera i cu abordul clasic.
miniinvazive laparoscopice oferă noi posibilită i
Concluzie: Apendicectomia laparoscopică la obezi
operatorii, cu avantaje evidente fa ă de cele clasice. Acest
este o alternativă viabilă, cu posibilitatea conversiei în
studiu retrospectiv este efectuat pe două loturi de
situa ii operatorii di cile.
pacien i obezi apendicectomiza i, unul prin procedeul
Cuvinte
cheie:
apendicectomie
clasică,
clasic și al doilea laparoscopic. S-au comparat aspectele
apendicectomie laparoscopică, apendicită, obezitate
intraoperatorii și evolu ia postoperatorie pentru a putea
aprecia varianta optimă de tratament.
Introducere
Material și metode: În perioada 2004-2013 s-a
efectuat apendicectomie clasică unui lot de
49 de
Apendicita acută este considerată aprioric o
pacien i obezi și laparoscopică unui lot de 24 de pacien i
interven ie simplă în chirurgia abdominală, ind
obezi. Am analizat comparativ durata interven iei,
realizată de mai bine de un secol [1] pe cale clasică, prin
durerea postoperatorie, complica iile postoperatorii,
incizie McBurney, cu rezultate bune. În ultimii 30 de
durata și costurile de spitalizare pentru a eviden ia
ani introducerea pe scară largă a tehnicilor laparoscopice
poten ialele bene cii ale laparoscopiei comparativ cu
miniinvazive a oferit o nouă op iune și pentru
abordul deschis în apendicita la obezi.
tratamentul
afec iunilor
apendiculare
prin
Rezultate: Durata medie a interven ei chirurgicale
apendicectomia laparoscopică. Chirurgia laparoscopică
a fost ușor mai mare pentru interven ia laparoscopică
s-a impus ca e cien ă în patologiile veziculei biliare,
Appendectomy in Obese People. Classic or Laparoscopic Approach?
97
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
colonului, rectului, ginecologice și a herniilor diverse. În
Rezultate
ceea ce privește apendicectomia, se constată o oarecare
rezisten ă din partea chirurgilor, cel pu in în România
Date generale
[2]. Pacien ii obezi reprezintă o categorie aparte fa ă de
Reparti ia pe sexe și pe grupe de vârstă a fost similară
cei
normoponderali
prezentând
problemele
în cele două loturi, cu o ușoară predominan ă a femeilor
comorbidită ilor frecvente, cum ar
afec iunile
și a decadelor a doua și a treia de via ă. Prevalen a bolilor
cardiovasculare și respiratorii, sau diabet zaharat. Riscul
asociate a fost de 28,6% la lotul cu interven ie clasică,
anestezic asociat este mult mai mare, necesitând o
respectiv
33,3% la cei cu interven ie laparoscopică
pregătire preoperatorie mai laborioasă [3]. Din punct de
(p=0,319), (Tabelul I).
vedere chirurgical, în cazul pacien ilor obezi, manevrele
Anestezia utilizată în lotul cu interven ie clasică a fost
operatorii sunt mult îngreunate de grosimea peretelui
rahidiană în 31 cazuri (63,3%), iar cea generală IOT în
abdominal care necesită incizii mai largi în chirurgia
18 cazuri (36,7%), în timp ce la interven ia laparoscopică
deschisă și de volumul mare de grăsime peritoneală care
s-a utilizat doar anestezia generală (100,0%) (Tabelul II).
acoperă câmpul operator [4]. Aceste impedimente au
Calea de abord pentru pacien ii opera i clasic a fost
determinat în chirurgia laparoscopică di cultă i în
incizia McBurney lărgită în 43 de cazuri și laparotomie
introducerea
primului
trocar,
insu area
mediană în alte trei, asociate cu o sarcină extrauterină
pneumoperitoneului, ventila ia pacientului după
ruptă, o ocluzie intestinală prin bridă și respectiv o
pozi ionarea în Trendelenburg și vizualizarea îngreunată
pelviperitonită. În lotul al doilea s-a efectuat apendicectomie
de grăsimea epiploică [5,6].
laparoscopică cu trei trocare în 23 de cazuri și într-un caz
Scopul studiului nostru a fost de a eviden ia
s-a efectuat unei paciente apendicectomie SILS prin abord
poten ialele bene cii ale laparoscopiei comparativ cu
miniinvaziv unic transombilical.
abordul deschis în apendectomia la obezi, bazându-ne
Durata inteven iei a fost cuprinsă între
31-150
pe experien a acumulată în ultimii 5 ani în serviciul
minute în opera ia clasică, rezultând o medie de 48
nostru, prin introducerea abordului laparoscopic în
minute și între 30-90 minute rezultând o medie de 51
apendicita acută, cu posibilitatea de conversie facilă la
minute la interven ia laparoscopică (Tabelul III).
chirurgia deschisă în cazurile complicate.
Administrarea de opiacee în prima zi postoperator
s-a făcut la 44 cazuri din lotul cu interven ie clasică
Material şi metode
(89,8%) și la 10 cazuri în cea laparoscopică (41,7%).
Dintre pacien ii apendicectomiza i am selectat pe cei
obezi cu un indice de masă corporală (IMC) mai mare de
Tabel I. Distribu ia cazurilor
30, opera i în perioada
2004-2013 de către același
în func ie de bolile asociate
colectiv chirurgical. Am selectat două loturi: unul de 49
Clasic
Laparoscopic
Boli asociate
de pacien i opera i deschis, celălalt de 24 de pacien i
Nr.
% Nr.
%
opera i laparoscopic, la care am comparat durata
Boli cardiovasculare
10
20,4
4
16,7
opera iei, tipul de anestezie, necesarul de analgezice
Diabet zaharat
2
4,1
1
4,2
majore postoperator, complica iile postoperatorii, durata
Afec iuni respiratorii
8
16,3
5
20,8
de spitalizare și costurile. Ca inten ie operatorie, lotul
Total
14
28,6
8
33,3
laparoscopic a cuprins ini ial 38 de pacien i, însă la 14
din aceștia (36,8%) am decis convertirea la abord deschis
Tabel II. Distribu ia cazurilor
datorită disfunc iilor legate de aparatura de laparoscopie,
în func ie de tipul anesteziei
sau di cultă ilor tehnice operatorii. Aceștia au fost incluși
în lotul operat clasic. Șapte dintre pacien ii converti i au
Clasic
Laparoscopic
Anestezie
avut apendicită gangrenoasă sau peritonită.
Nr.
% Nr.
%
Datele au fost culese prin analiza foilor de observa ie
Rahidiană
31
63,3
0
0,00
ale pacien ilor, studiul protocoalelor operatorii, a bazei
Generală IOT
18
36,7
24
100,0
de date computerizate din spitale și prin examinarea
înregistrărilor video intraoperatorii. Datele pacien ilor
Tabel III. Durata medie a interven iei
au fost folosite cu acordul acestora și au fost tratate într-
un regim con den ial.
Clasică
Laparoscopică
Analiza statistică s-a făcut cu ajutorul aplica iei
Limite
31-150 min
30-90 min
EPIINFO 6.0 și a testului Student.
Durata medie
48±22 min
51±25 min
98
Sfîrlea et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
Analiza morfopatologică
Complica ii
Din cazurile con rmate de apendicită acută (36 din
Complica iile infec ioase precoce au fost
lotul cu interven ie clasică și 20 din cele cu interven ie
semni cativ mai frecvente la lotul cu apendicectomie
laparoscopică), majoritatea au fost catarale sau
clasică fa ă de metoda laporoscopică (73,3% vs. 22,7%)
egmonoase (55,6, respectiv 65,0%) (p=0,046).
(p<0,001). Cea mai frecventă complica ie precoce a fost
Apendicitele acute gangrenoase au fost prezente la
infec ia plăgii, întâlnită la
68,9% dintre pacien ii cu
25,0% din cazuri, respectiv
15,0%
(p=0,005),
apendicectomie clasică și la
18,2% dintre cei cu
peritonitele apendiculare în
13,9% din cazuri,
apendicectomie laparoscopică (p<0,001) (Tabelul VI).
respectiv 10,0% (p=0,195), iar blocul periapendicular
În ecare lot de pacien i obezi a fost câte un caz
abcedat a fost prezent la 5,6% cazuri, respectiv 10,0%
complicat cu abces intraperitoneal care a răspuns bine la
(p=0,142). Din punct de vedere statistic există
tratament conservator cu antibiotice. Un pacient operat
diferen e semni cative între cele două loturi în ceea ce
clasic a prezentat peritonită de ziua a
5-a, care s-a
privește tipul de apendicită acută (p=0,009) (Tabelul
rezolvat conservator.
IV).
Alte complica ii precoce postoperatorii s-au
Diagnosticul de apendicită acută nu a fost con rmat
înregistrat la 26,7% dintre cazurile cu apendicectomie
în 13 cazuri (26,5%) din lotul cu interven iei clasică și 4
clasică și la 18,1% la cei cu apendicectomie laparoscopică
cazuri (16,7%) din lotul cu interven ie laparoscopică.
(p=0,026). La lotul cu apendicectomie clasică cele mai
Dintre aceștia, majoritatea au avut apendice sănătos,
multe cazuri au fost de ileus precoce (4 cazuri - 8,9%),
fără modi cări macroscopice (46,2%, respectiv 50,0%)
din care 3 pacien i au fost rezolva i conservator, iar în
(p=0,447) (Tabelul V).
cazul unui pacient s-a reintervenit, practicându-se
Patologii asociate ginecologice, limfadenită
laparotomie mediană și adezioliză. Un singur caz din
mezenterică, colecistită acută sau ocluzie intestinală
lotul pacien ilor apendicectomiza i laparoscopic a
prin bride sau aderen e au prezentat 30,8% din cazurile
prezentat ileus postoperator, remis sub tratament
cu interven ie clasică, respectiv
50,0% din cea
conservator.
laparoscopică (p<0,001). În nal, apendicectomia s-a
Unul din cazurile operate clasic a prezentat
aplicat la 45 de cazuri din lotul cu interven ie clasică
hemoragie la nivelul peretelui abdominal exteriorizată la
(91,8%) și la
22 de cazuri din cele cu interven ie
dren, necesitând reinterven ia pe cicatricea McBurney.
laparoscopică (91,7%).
O pacientă operată prin abord median a prezentat o
Tabel IV. Distribu ia cazurilor în func ie de
Tabel VI. Distribu ia cazurilor în func ie de
tipul morfopatologic al apendicitei
complica iile infec ioase precoce
Clasică
Laparoscopică
Clasică
Laparoscopică
Morfopatologie
Complica ii precoce
Nr.
% Nr.
%
Nr.
% Nr.
%
Catarale sau egmonoase
20
55,6
13
65,0
Infec ii plagă
31
68,9
4
18,2
Gangrenoase
9
25,0
3
15,0
Abces profund
1
2,2
1
4,5
Peritonite apendiculare
5
13,9
2
10,0
Bloc periapendicular
Peritonite de ziua a 5-a
1
2,2
0
0,0
2
5,6
2
10,0
abcedat
Total
33
73,3
5
22,7
Total
36
100,0
20
100,0
Tabel V. Distribu ia diagnosticelor la cazurile la care
Tabel VII. Distribu ia cazurilor în func ie de
s-a in rmat intraoperator apendicita
alte complica ii precoce
Clasică
Laparoscopică
Alte complica ii
Clasică
Laparoscopică
Nr.
% Nr.
%
precoce
Nr.
% Nr.
%
Apendice sănătos
6
46,2
2
50,0
Hemoragie
1
2,2
0
0,0
Patologie ginecologică
4
30,8
2
50,0
Ileus precoce
4
8,9
1
4,5
Ocluzie/bride
1
7,7
0,0
Eviscera ie
1
2,2
0
0,0
Colecistită
1
7,7
0,0
Infec ii respiratorii
3
6,7
1
4,5
Limfadenita mezenterică
1
7,7
0,0
Infec ii urinare
3
6,7
2
9,1
Total
13
100,0
4
100,0
Total
12
26,7
4
18,1
Appendectomy in Obese People. Classic or Laparoscopic Approach?
99
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
eviscera ie la polul inferior al plăgii pentru care a fost
apărare imună, reprezintă locul de elec ie pentru
necesară reinterven ia sub anestezie generală (Tabelul
însămân area germenilor din peritoneu și predispune la
VII).
infec ii postoperatorii. Lungimea mult mai mică a
Complica iile tardive s-au constatat în cazurile
inciziilor la nivelul peretelui adipos și traumatizarea
prezentate la control în clinica noastră, care au necesitat
redusă a acestuia prin utilizarea trocarelor, precum și
tratament chirurgical.
lipsa contactului direct cu apendicele infectat în cursul
La lotul cu apendicectomie clasică, s-au înregistrat 6
manevrelor de extrac ie a acestuia explică frecven a mult
cazuri cu complica ii tardive
(13,3%), dintre care 4
mai mică a infec iilor parietale (73,3% vs. 22,7%). Au
cazuri de eventra ie (8,9%), 3 pe incizie McBurney și
existat câte un caz de abces profund postoperator și o
unul pe laparotomie mediană. Alte 2 cazuri au necesitat
peritonită de ziua a 5-a, care au fost rezolvate conservator.
reinterven ia pe linie mediană pentru sindrom aderen ial
Aceste rezultate sunt asemănătoare cu cele descrise în
(4,4%). La lotul cu apendicectomie laparoscopică s-a
literatură [6,7].
înregistrat un singur caz cu o complica ie tardivă, o
Durata medie de spitalizare la pacien ii cu
pacientă cu sindrom aderen ial postoperator pentru care
interven ie clasică a fost aproape dublă fa ă de cea
s-a făcut adezioliză laparoscopică
(4,5%) (p<0,001),
înregistrată la pacien ii cu interven ie laparoscopică (6,2
(Tabelul VIII).
zile vs. 3,3 zile) (p<0,001). Acest lucru se datorează în
special apari iei complica iilor precoce postoperator,
Tabel VIII. Distribu ia cazurilor în func ie de
semni cativ mai frecvente în cazul interven iei clasice,
complica iile tardive
dar și recuperării mai lente postoperator a pacien ilor
obezi opera i prin laparotomie.
Clasică
Laparoscopică
Complica ii tardive
Am calculat costurile luând în considerare numărul
Nr.
% Nr.
%
mediu de zile de spitalizare a pacien ilor din cele două
Eventra ie
4
8,9
0
0,0
grupuri de obezi, precum și a consumului de
Sindrom aderen ial
2
4,4
0
0,0
Ocluzie/bridă
0
0,0
1
4,5
medicamente, de investiga ii imagistice și diferitele
Total
6
13,3
1
4,5
tipuri de anestezie utilizate.
Contrar rezultatelor din literatură
[8,9], costul
mediu/caz a fost mai mare la lotul cu interven ie clasică
(2.253 lei vs. 1.955 lei), diferen ă datorată în special
Discuții
complica iilor, care au necesitat mai multe zile de
internare la terapie intensivă și medica ie complexă, dar
Câteva dintre rezultatele ob inute prin prezentul
și un număr mai mare de zile de spitalizare.
studiu merită o aten ie deosebită. Astfel, aproximativ o
Trebuie să men ionăm că nu am introdus în calcul
treime dintre pacien i, majoritatea sub 40 de ani, a
amortizarea instrumentelor de laparoscopie, care
prezentat patologie asociată cardiacă, respiratorie sau
reprezintă o pondere anciară importantă, iar costul
diabet zaharat, ilustrând di cultă ile legate de chirurgia
materialelor consumabile a fost nesemni cativ. Nu am
la obezi. Un alt aspect important este legat de durata
utilizat endostaplere pentru ligatura apendicelui și a
interven iei chirurgicale, unde nu s-au înregistrat
mezoului său, ci endolupe preînodate de noi cu r de
diferen e semni cative (48 vs. 51 de minute), aceasta
Biocryl
2-0, iar pentru extrac ia apendicelui am
putând explicată prin timpii mai lungi necesari pentru
improvizat endobag-uri din mănușă chirurgicală.
laparotomie
(în
3 cazuri mediană subombilicală) și
Apendicectomia laparoscopică la obezi este asociată
pentru închiderea peretelui la obezi, comparativ cu cei
cu mai pu ine complica ii postoperatorii decât cea
necesari pentru introducerea trocarelor.
deschisă, însă rata de abcese profunde postoperatorii este
Durerea postoperatorie apreciată prin necesarul de
cu pu in mai mare (4,5 vs. 2,2%), rezultate ce coincid cu
medicamente opiacee administrate postoperator a fost
majoritatea studiilor publicate. Timpul operator mediu
mai redusă în cazul pacien ilor opera i laparoscopic, în
este nesemni cativ mai mare pentru pacien ii cu
mod evident datorită traumatismului parietal mai
laparoscopie
(51 vs.
48 minute). Durata medie de
mic.
spitalizare a fost mai redusă fa ă de cea a pacien ilor
Dintre complica iile precoce, cele mai studiate și
opera i deschis
(6,2 vs.
3,3 zile). Prin excluderea
mai frecvente în literatură sunt cele infec ioase precoce,
cheltuielilor de amortizare a aparaturii de laparoscopie,
care pot super ciale, la nivelul plăgii, sau profunde. La
costul mediu de spitalizare a fost mai avantajos pentru
obezi, esutul adipos mult mai abundent, cu o
opera iile laparoscopice. La interpretarea acestor rezultate
vasculariza ie mai redusă și o capacitate mai redusă de
trebuie să inem cont de faptul că 14 din pacien ii la care
100
Sfîrlea et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
s-a tentat abordul laparoscopic au fost incluși în lotul de
4.
Mason RJ, Mason AJ. Open-close case? New data on
49 de pacien i opera i clasic datorită di cultă ilor tehnice
appendectomy in an obese patient cohort. Expert Rev
intraoperatorii, 7 dintre aceștia suferind de apendicite
Gastroenterol Hepatol 2013;7(1):1-3.
gangrenoase sau perforate cu in ama ii severe
5.
Corneille MG, Steigelman MB, Myers JG, Jundt J,
periapendiculare.
Dent DL et al. Laparoscopic appendectomy is superior
to open appendectomy in obese patients. Am J Surg
Concluzie
2007;194(6):877-80.
6.
Mason RJ, Moazzez A, Moroney JR, Katkhouda N.
Apendicectomia laparoscopică la obezi reprezintă o
Laparoscopic vs open appendectomy in obese patients:
variantă operatorie avantajoasă pacientului, cu rezerva
outcomes using the American College of Surgeons
posibilită ii de conversie la chirurgia clasică în cazurile
National Surgical Quality Improvement Program
complicate.
database. J. Am Coll Surg
2012;215(1),
88-99;
discussion 99.
7.
Gaszynski T.
e e ect of pneumoperitoneum on
Referințe
haemodynamic parameters in morbidly obese patients.
Anestezjol Intens Ter 2011;43(3):148-52.
1. McBurney C. e incision made in the abdominal wall
8.
Gorenoi V, Dintsios CM, Schönermark MP, Hagen
in cases of appendicitis, with a description of a new
A. Laparoscopic vs. open appendectomy: systematic
method of operation. Ann Surg 1894;20:38-43.
review of medical e cacy and health economic analysis.
2. Nicolau A E. Apendicectomia laparoscopică Chirurgia
GMS Health Technol Assess 2007;2:Doc22.
2011;106:495-503.
9.
Kehagias I, Karamanakos SN, Panagiotopoulos S,
3. Dority J, Hassan ZU, Chau D. Anesthetic implications
Panagopoulos K, Kalfarentzos F. Laparoscopic versus
of obesity in the surgical patient. Clin Colon Rectal
open appendectomy: which way to go? World J
Surg. 2011 ;24(4):222-8.
Gastroenterol 2008;14(31):4909-14.
Appendectomy in Obese People. Classic or Laparoscopic Approach?
101
Ion IC Brătianu Blvd, at the corner with Eugen Lovinescu St.
(Bulevardul Ion IC Brătianu, col cu strada Eugen Lovinescu)
e Postal O ce building, Jean Calvin Square at the corner with
General Alexandru Averescu St. (Clădirea Poştei, Pia a Jean Calvin,
col cu strada General Alexandru Averescu)
ORIGINAL ARTICLES
INCIDENȚA DRENAJULUI LIMFATIC ATIPIC LA PACIENȚII CU MELANOM
MALIGN
Florin Suru, Adrian Maghiar
Catedra de Chirurgie, Facultatea de Medicină şi Farmacie, Universitatea Oradea
Adresa pentru coresponden ă:
Florin Suru
Tel. 0744760240
E-mail:
_suru@yahoo.com
Primit: 15.01.2014
Acceptat: 28.02.2014
Med Con March 2014, Vol 9, No 1, 103-107
Rezumat
Melanoamele de pe extremită i au arătat drenaj spre
SLN atipic în 4 (16,66%) din 24, respectiv 3 (6,38%)
Ganglionii limfatici regionali care drenează din
din 47 de pacien i pentru membrele superioare, respectiv
melanomul primar reprezintă locul comun de
inferioare. Inciden a generală de drenaj limfatic atipic a
metastazare ini ială la pacien ii în stadiile I și II de boală.
fost de 18,83% (29 de pacien i din totalul de 154).
Prin urmare, localizarea precisă și stadializarea
Concluzii: Drenajul atipic este mai frecvent în
ganglionilor limfatici de drenaj sunt cruciale în
cazul melanoamelor capului și gâtului, urmat de cele de
tratamentul acestor pacien i. Studiile limfoscintigra ce
pe trunchi. Limfoscintigra a preoperatorie permite
au demonstrat variabilitatea modelelor de drenaj
de nirea unor modele de drenaj individuale, personale,
limfatic din diferite reguni de melanom malign primar.
contribuind astfel în mare parte la succesul disec iei
Obiectiv: Corelarea modelelor de drenaj limfatic
selective de nod limfatic santinelă.
din următoarele trei surse: predic ie clinică preoperatorie
Cuvinte cheie: melanom malign, limfoscintigra e,
bazată pe localizarea anatomică a tumorii primare,
nodul limfatic santinelă, drenaj limfatic atipic
modelul de drenaj limfatic determinat de
limfoscintigra a preoperatorie și identi carea nodulului
Introducere
limfatic santinelă
(SLN) în cursul interven iei
chirurgicale.
Nodulii limfatici regionali care drenează din
Material și metodă: Limfoscintigra a preoperatorie
melanomul primar sunt cele mai comune locuri de
a fost efectuată pe 154 de pacien i interna i și opera i pe
metastazare ini ială la pacien ii în stadiile I și II de boală
sec ia de Chirurgie Oncologică a Spitalului Municipal
[1]. Prin urmare, localizarea precisă și stadializarea
Timișoara cu diferite stadii de melanom malign primar.
nodulilor limfatici de drenaj sunt cruciale în tratamentul
Rezultate: Limfoscintigra a preoperatorie a
acestor pacien i.
identi cat cel pu in un SLN pentru to i pacien ii incluși
În mod tradi ional, nodulii limfatici de drenaj au
în studiu.
6 (33,33%) pacien i cu melanoame ale
fost diseca i în scopuri pro lactice. Bazinele disecate în
capului și gâtului dintre cei
18 pacien i analiza i au
disec ia electivă a nodului limfatic s-au bazat pe modelele
prezentat cel pu in 1 SLN în afara zonelor anticipate
anatomice de coloid de drenaj limfatic cutanat pe
clinic. Discordan a pentru melanoamele de trunchi a
cadavre descris de Sappey [2] și modi cate de Sugarbaker
fost observată în
16
(24,61%) din
65 de cazuri.
și McBride [3], bazate pe modele clinice.
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
103
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Dezvoltarea tehnicii de disec ie selectivă a nodulului
Ca o descriere scurtă a tehnicii limfoscintigra ei:
limfatic santinelă
(SSLND) pentru pacien ii cu
technetium Tc 99m (99mTc) sulfuric coloid ltrat printr-
melanom reprezintă un progres major în tratamentul
un ltru de 22 µm a fost injectat intradermic în jurul
acestora [4]. Numeroase studii au constatat că starea
tumorii primare sau a cicatricii după biopsie. Cu
SLN prezice în mod sigur starea bazinului nodal [5].
ajutorul camerei gamma-cap dublu (ADA Vertex) se
Această tehnică minim invazivă permite evaluarea
ob in imediat imagini dinamice pentru a evalua
patologică a SLN. Când rezultatele evaluării patologice
absorb ia radiotrasorului în căile limfatice. Imaginile
sunt negative nu mai este necesară disec ia nodulilor
întârziate se înregistrează de la 20 de minute până la 2
limfatici din bazin [6]. Cu toate acestea, precizia tehnicii
ore pentru depistarea tuturor bazinelor predispuse
SSLND depinde de abilitatea localizării preoperatorie
instalării metastazelor și a studierii asimilării substan ei
limfoscintigra ce a SLN. Limfoscintigra a s-a dovedit a
radiocoloidale prin vizualizarea urmelor în
cat.
un excelent predictor al drenajului limfatic de la
Localizarea SLN se marchează pe piele cu colorant
melanomul primar bazat pe recuren e nodale, fapt
(cerneală neradioactivă).
demonstrat prin urmărire pe termen lung [7].
Înainte de începerea interven iei chirurgicale se
Studiile limfoscintigra ce timpurii au demonstrat
injectează limfazurin albastru - Bleu Patent (1% într-o
variabilitatea modelelor de drenaj limfatic din diferite
solu ie apoasă) în jurul melanomului primar, sau în
regiuni de melanom malign primar. Deși regiunea
jurul locului unde a fost făcută biopsia (aproximativ 4
capului și gâtului pare să arate cea mai mare variabilitate
puncte).
[8], regiunea toracelui demonstrează, de asemenea,
Procedura disec iei selective de nodul limfatic
varia ii semni cative
[9,10], în special pentru
santinelă este asociată unei largi excizii locale a tumorii
melanoamele apărute pe linia mediană și în apropierea
primare. Folosind o sonda gamma manuală (Neoprobe
liniei Sappey. Drenajul de la melanoamele extremită ilor
Corporation, Dublin, Ohio) se localizează nodulii
a fost considerat a mai pu in variabil.
limfatici cu emisii ridicate gamma. Pentru identi carea
Limfoscintigra a preoperatorie și intraoperatorie
exactă a SLN s-au folosit ratele înalte de semnal nodul-
prin cartogra erea SLN poate constitui o alternativă
fundal
[12], sau colora ia în albastru a nodulilor
preferată la metoda tradi ională de disec ie electivă a
limfatici.
nodulului bazată pe predic ii preoperatorii anatomice
Predic ia clinică a localizării bazinelor limfatice de
[11]. Limfoscintigra a preoperatorie va identi ca cu
drenaj din locul tumorii primare s-a făcut conform
mare precizare drenarea bazinului nodal, după care
modelelor standard de drenaj. Pentru membrele
cartogra erea intraoperatorie a SLN va facilita SSLND
inferioare, drenajul limfatic din zona cutanată este
pentru stadializarea corectă a bazinului nodal, scutind
așteptat în aria inghinală (femurală). Drenajul în aria
astfel aproximativ
80% din pacien ii cu melanom
poplitee a fost considerat atipic. Pentru membrele
malign de o disec ie limfatică electivă inutilă [4].
superioare singura zonă presupusă a fost cea axilară.
Obiectivul studiului este de a evalua inciden a
Drenajul în zonele epitrohleare sau supraclaviculare au
drenajului limfatic neconcordant cu modelul anatomic
fost considerate atipice.
clasic la pacien ii cu melanom malign invaziv. În acest
Pentru pacien ii cu melanoame pe trunchi drenajul
sens au fost comparate rezultatele cartogra erii
limfatic este așteptat în cea mai apropiată zonă inghinală
drenajului limfatic prin limfoscintigra e pre- și
sau axilară [2,3]. Dacă tumora primară a fost localizată
intraoperatorie cu modelele tradi ionalele anatomice și
sub 2,5 cm de linia mediană, drenajul poate apărea pe
cele cu predic ii clinice.
oricare parte sau bilateral, ne ind considerat atipic.
Similar, pentru melanomele primare situate sub 2,5 cm
Material şi metodă
de linia Sappey, drenajul poate apărea în zonele
ipsilaterale inghinal sau axilar, sau ambele. De exemplu,
Pacien ii pentru acest studiu observa ional,
o tumoră primară localizată în jurul ombilicului sau în
retrospectiv și prospectiv, de cohortă, au fost selecta i
aria L2 poate drena în orice combina ie de bazine
dintre bolnavii interna i pe Sec ia de Chirurgie
inghinale sau axilare, fără să e considerată atipică.
Oncologică a Spitalului Municipal Timișoara pentru
Pentru bolnavii cu melanom malign primar localizat
melanom malign invaziv în perioada 2001-2013.
la nivelul capului sau gâtului, algoritmul de detectare a
To i bolnavii care au fost supuși biopsiei de tumoră
drenajului aberant s-a bazat direct pe modelul ilustrat de
primară și disec iei selective de SLN în urma
O’Brien și colab. [8]. Leziunile primare au fost clasi cate
limfoscintigra ei, au fost identi ca i. Au fost excluși
după loca ie în 10 regiuni ale capului și gâtului. Ariile de
pacien ii sub 18 ani și gravidele.
drenaj identi cate au fost: parotidiană
(aria
1),
104
Suru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
submandibulară sau triunghiul submentonier (aria 2),
Tabel I. Ariile de drenaj corespunzătoare
jugulară superioară (aria 3), jugulară mijlocie (aria 4),
regiunilor tumorii primare
jugulară inferioară (aria 5), triunghiul posterior (aria 6) și
Aria anticipată
Localizare tumoră primară
zona occipitală (aria 7). Dacă o tumoră primară a arătat
de drenaj
drenaj limfatic în afara ariei de predic ie, acel drenaj a
Scalp anterior
1-4
fost considerat atipic. Ariile de drenaj corespunzătoare
Scalp coronal (bandă de 5 cm)
1-6
regiunilor tumorii primare sunt prezentate în Tabelul I.
Scalp posterior
2-5,7
Fa ă
1-4
Criteriile urmărite în acest studiu au fost numărul și
Ureche
1-6
localizarea SLN pentru ecare pacient în parte și
Gât antero-superior
1-5
compararea acestora cu modelul de drenaj anatomic
Gât coronal (bandă de 5 cm)
1-6
descris anterior. În afară de aceste date au mai fost
Gât postero-superior
2-5,7
notate: vârsta, sexul, nivelul de invazie Clark, grosimea
Gât antero-inferior
3-5
pe scala Breslow și rezultatul histopatologic al SLN.
Gât postero-inferior
3-5
Rezultate
Tabelul II. Numărul de SLN identi cate intraoperator
Numărul pacien ilor care au îndeplinit criteriile de
Număr SLN
Nr. pacien i Procent (%)
p*
includere și excludere din acest studiu a fost de 154.
identi ca i
Dintre aceștia au fost 60 (39%) de bărba i și 94 (61%)
0
5
3,2%
de femei, cu o vârstă medie de
53,9 ani
(Devia ia
1
115
74,7%
Standard=13,45).
2
26
16,9%
<0,0001
Grosimea medie a melanomului primar măsurat pe
3
4
2,6%
scala Breslow a fost de 2,53 mm (DS=1,43), cu nivel
4
4
2,6%
median de invazie Clark de 3 (IC95%=3-4).
* testul chi-pătrat
Tabel III. Cazuri de atipie, analizând rezultatele limfoscintigra ei
împreună cu modelele de drenaj limfatic predictive
Localizarea tumorii primare şi modelul de drenaj limfatic
Cauza drenajului atipic
Număr de cazuri
Cap şi gât (n=18)
Standard
Fără
12
Drenaj într-o arie neconformă ariei anticipate*
Drenaj atipic
6
Trunchi (n=65)
Standard
Fără
49
Axilar contralateral
Drenaj peste linia mediană
6
Inghinal contralateral
Drenaj peste linia mediană
1
Cervical anterior şi/sau posterior
Drenaj atipic
2
Supraclavicular
Drenaj atipic
3
Perete toracic
Drenaj atipic
2
Lombar inferior
Drenaj atipic
1
Triunghi posterior
Drenaj atipic
1
Extremită i superioare (n=24)
Axilar
Fără
20
Axilar şi epitrohlear
Bazin adi ional
1
Axilar şi supraclavicular
Bazin adi ional
1
Axilar şi subclavicular
Bazin adi ional
1
Numai supraclavicular
Drenaj atipic
1
Extremită i inferioare (n=47)
Inghinal
Fără
44
Inghinal şi popliteu
Bazin adi ional
3
* vezi Tabelul I
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
105
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
examenul histopatologic este ușor crescută fa ă de studiile
asemănătoare [13], ceea ce se explică probabil și prin
faptul că pacien ii au prezentat o boală mai avansată în
momentul internării fa ă de loturile studiate în literatură.
În schimb inciden a generală și reparti ia pe
regiunile corpului a cazurilor de drenaj limfatic atipic
din melanomul primar au fost comparabile cu datele
din literatură [14].
Concluzii
Limfoscintigra a preoperatorie este o condi ie
Figura 1. Inciden a apari iei drenajului atipic
esen ială pentru o disec ie selectivă de SLN.
În cazul melanoamelor de pe extremită i, metoda
To i pacien ii au fost supuși limfoscintigra ei,
permite identi carea rară a drenajului spre alte bazine
identi cându-se cel pu in un bazin de SLN preoperator.
decât cele axilare și inghinale. Pentru tumorile primare
Tabelul II arată numărul de SLN identi cate
localizate pe trunchi, modelele de drenaj standard pot
intraoperator.
include bazine ipsilaterale sau bilaterale, iar drenajul
În ceea ce privește rezultatul histopatologic, din
atipic poate implica noduli în tranzi ie, sau noduli de
totalul de 154 de pacien i, 61 (39,6%) de bolnavi au
drenaj neobișnui i. Drenajul melanoamelor localizate pe
fost găsi i cu micrometastaze la nivelul SLN diseca i.
pielea capului și gâtului este foarte variabil, iar
Acești pacien i au suferit o evidare ganglionară extensivă.
limfoscintigra a oferă o armă importantă care să ghideze
Analizând rezultatele limfoscintigra ei împreună cu
chirurgul spre ariile care drenează un anumit melanom
modelele de drenaj limfatic predictive s-au observat
primar.
cazuri de atipie (Tabel III).
Limfoscintigra a preoperatorie permite de nirea
Inciden a apari iei drenajului atipic respectă datele
unor modele de drenaj individuale, personale,
din literatură, ind cea mai frecventă la nivelul capului,
contribuind astfel în mare parte la succesul disec iei
gâtului și trunchiului
(p=0,0330, testul chi-pătrat),
selective de nodul limfatic santinelă.
Figura 1.
Inciden a generală de drenaj limfatic atipic a fost de
18,83% (29 de pacien i din totalul de 154 de cazuri).
Referințe
Discuții
1. Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic
factor analysis of 17,600 melanoma patients: validation
Studiul nostru a eviden iat că la majoritatea
of the American Joint Committee on Cancer melanoma
pacien ilor numărul SLN identi ca i intraoperator a
staging system. J Clin Oncol 2001;19:3622-3634.
fost de
1 sau
2, iar prezen a micrometastazelor de
2. Sappey MPC. Anatomie, Physiologie, Pathologie des
melanom malign a fost de aproape 40% din cazuri.
Vaisseaux Lymphatiques Conside´re´s Chez l’Homme et
Comparând frecven a drenajului atipic pentru
les Verte´bre´s. Paris, France: DeLahaye A, Lecrosnier
diferite localizări a melanomului primar se constată
E; 18[74]85.
predominen a acestuia în cazul tumorilor primare de pe
3. Sugarbaker EV, McBride CM. Melanoma of the trunk:
trunchi, cap și gât care reprezintă mai mult de 55% din
the results of surgical excision and anatomic guidelines
cazurile de drenaj atipic.
for predicting nodal metastasis. Surgery 1976; 80:22-
Valoarea ridicată a inciden ei generale a drenajului
30.
limfatic atipic conferă limfoscintigra ei o importan ă
4. Leong SPL. e role of sentinel lymph node in human
deosebită în cartogra erea SLN.
solid cancer. In: Devita VT, Hellman S, Rosenberg
Din această analiză s-a eviden iat clar că în lipsa
SA, eds. PPO Updates. Philadelphia, Pa: Lippincott-
limfoscintigra ei și a cartogra erii exacte a drenajului
Raven Publishers; 1998:1-12.
limfatic individualizat pentru ecare pacient, riscăm ca
5. Morton DL, ompson JF, Cochran AJ, et al. Sentinel
adevăratul SLN să nu e identi cat și disecat.
node biopsy or nodal observation in melanoma. N Engl
Aceste rezultate se apropie de observa iile studiilor
J Med 2006; 355:1307-17.
din literatură. Inciden a nodulilor limfatici pozitivi la
6. Clary BM, Brady MS, Lewis JJ, Coit DG. Sentinel
106
Suru et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
ORIGINAL ARTICLES
lymph node biopsy in the management of patients with
eds. Cutaneous Melanoma. 2nd ed. Philadelphia, Pa:
primary cutaneous melanoma: review of a large single-
Williams&Wilkins; 1992:367-75.
institutional experience with an emphasis on recurrence.
11.
ompson JF, Uren RF, Shaw HM, et al. Location of
Ann Surg 2001;233:250-8.
sentinel lymph nodes in patients with cutaneous
7. Berger D, Feig B, Podolo D, et al. Lymphoscintigraphy
melanoma: new insights into lymphatic anatomy. J Am
as a predictor of lymphatic drainage from cutaneous
Coll Surg 1999; 189:195-206.
melanoma. Ann Surg Oncol 2004; 4:247-51.
12. Albertini JJ, Cruse WC, Rapaport D, et al.
8. O’Brien CJ, Uren RF, ompson JF, et al. Prediction
Intraoperative
radiolymphoscintigraphy
improves
of potential metastatic sites in cutaneous head and neck
sentinel lymph node identi cation in melanoma. Ann
melanoma using lymphoscintigraphy. Am J Surg 1995;
Surg 1996;223:217-24.
170:461-6.
13. Karim RZ, Scolyer RA, Li W, et al. False negative
9. Uren DF, Howman-Giles RB, Shaw HM, ompson
sentinel lymph node biopsies in melanoma may result
JF, McCarthy WH. Lymphoscintigraphy in high risk
from de ciencies in nuclear medicine, surgery, or
melanoma of the trunk: predicting draining node groups,
pathology. Ann Surg 2008;247:1003-10.
de ning lymphatic channels and locating the sentinel
14. Gershenwald JE, ompson W, Mans eld PF, et al.
node. J Nucl Med 1993; 34:1435-40.
Multi-institutional melanoma lymphatic mapping
10. Lamki LM, Logic JR. De ning lymphatic drainage
experience: the prognostic value of sentinel lymph node
patterns with cutaneous lymphoscintigraphy. In: Balch
status in 612 stage I or II melanoma patients. J Clin
CM, Houghton AN, MiltonGW, Sober AJ, Soong SJ,
Oncol 1999;17: 976-83.
Incidence of Atypical Lymphatic Drainage in Patients with Malignant Melanoma
107
Crossroad of the Miori ei Street with the Corvinilor Street
(intersec ia străzii Miori ei cu strada Corvinilor)
Crossroad of the Vasile Lucaciu Boulevard with the
Ion IC Brătianu Boulevard, 1943 and today
(intersec ia bulevardului Vasile Lucaciu cu bulevardul
Ion IC Brătianu, în 1943 şi azi)
CASE PRESENTATION
SINDROMUL NEFROTIC ŞI INSUFICIENȚA RENALĂ ACUTĂ CAUZATE
DE LEUCEMIA LIMFOCITARĂ CRONICĂ. PREZENTARE DE CAZ ŞI O
REVISTĂ A LITERATURII
Boris Solun1, Dana Marcoviciu1, Yulia Belnik1, Avraham Sendovski1, Dror Dicker1, Ana Tovar2
Departmentele de 1Medicină Internă D şi de 2Patologie, Centrul Medical Rabin, Petah Tikva, a liat Facultă ii de
Medicină Sackler, Universitatea Tel Aviv, Tel Aviv, Israel
Adresa pentru coresponden ă:
Dr. Boris Solun
Department of Internal Medicine D
Rabin Medical Center - Hasharon Hospital
7 Keren Kayemet St., Petach Tikva 49100, Israel
Tel: 972-3- 9372426, Fax: 972-3-9372427
E-mail: bsolun@gmail.com
Primit: 14.01.2014
Acceptat: 15.02.2014
Med Con March 2014, Vol 9, No 1, 109-114
Rezumat
ca o consecin ă a hipogammaglobulinemiei şi a
tratamentului cu imunosupresoare şi anticorpi
Implicarea renală în leucemia limfocitară cronică
monoclonali.
(LLC), nu este neobişnuită şi de obicei se datorează
Cuvinte cheie: leucemie limfocitară cronică,
in ltrării renale de către celulele leucemice. Cu toate
sindrom nefrotic, tratament
acestea, LLC asociată cu proteinuria datorată afectării
Abrevieri: LLC, leucemie limfocitarăcronică;
glomerulare prin sindromul nefrotic apare la doar 1%-
MPGN, glomerulonefrită membranoproliferativă
2% dintre pacien i. Raritatea glomerulopatiei în acest
context sugerează că celulele tumorale pot avea anumite
Introducere
proprietă i care conduc la dezvoltarea glomerulonefritei.
Scopul acestui raport este de a descrie un pacient cu
Leucemia limfocitară cronică
(LLC) se poate
LLC, insu cien ă renală acută, sindrom nefrotic şi
complica cu insu cien ă renală acută, de obicei ca
crioglobulinemie. Biopsia medulară a relevat răspândirea
urmare a in ltrării rinichiului de către celulele leucemice.
difuză a unui mare număr de limfocite mici, compatibile
Cu toate acestea, in ltrarea tumorală directă şi
cu diagnosticul de LLC. Biopsia renală a demonstrat un
proliferarea celulelor B, cu afectarea ulterioară
model de glomerulonefrită membranoproliferativă, cu
glomerulară sub forma proteinuriei sau sindromului
leziuni exudative şi de necroză consistente cu
nefrotic, apare doar la 1% până la 2% din pacien i.
crioglobulinemia. Tratamentul combinat cu rituximab,
Această asociere a fost descrisă pentru prima dată de
dexametazonă şi clorambucil a condus la o ameliorare
către Scott în 1957 [1,2]. Cea mai frecventă leziune în
atât a func iei renale cât şi a proteinuriei, con rmând
sindromul
nefrotic
este
glomerulonefrita
natura paraneoplazică a afectării glomerulare. Pacienta a
membranoproliferativă (MPGN) [3]. Crioglobulinemia,
decedat prin complica ii ale pneumoniei câteva luni mai
predominant de tip I, a fost implicată în legătura dintre
târziu. Infec iile, de obicei, de origine bacteriană, sunt o
MPGN şi LLC [4]. Raritatea glomerulopatiei la
complica ie importantă în managementul LLC, apărând
pacien ii cu LLC poate indica un sindrom paraneoplazic.
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
109
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Această ipoteză este sus inută de ameliorarea substan ială
Analizele sangvine: hemoglobina 7,3 g/dl (12 g/dl
a ambelor afec iuni prin chimioterapie [5,6]. Scopul
înainte cu cinci luni), numărul de leucocite şi trombocitele
acestei prezentări este de a descrie cazul unei paciente cu
au fost în limite normale. Creatinina serică a fost 2,7 mg/
LLC, insu cien ă renală acută, sindrom nefrotic şi
dl (0,8 mg/dl anterior cu cinci luni), uree 145,8 mg/dl,
crioglobulinemie.
sodiu 142 mEq/l, potasiu 7,19 mEq/l, clor 117,9 mEq/l,
calciu 7,7 mg/dl, acid uric 6,6 mg/dl, albumină 2,9 g/dl.
Prezentare de caz
Testele func ionale hepatice, timpul de protrombină şi
timpul de tromboplastină par ial activată au fost în limite
O femeie de origine evreiască, în vârstă de 79 de
normale. Electrocardiograma a relevat ritm sinusal
ani, a fost internată prezentând astenie, edeme ale
normal, cu unde T mari, înalte, subdenivelarea
membrelor inferioare, gre uri şi pierdere în greutate de
segmentului ST în deriva iile V1-V2. Analiza urinei (pe
aproximativ 4 kg în ultima lună, fără febră. Antecedentele
strip) a arătat proteine pozitive, cu un număr mare de
au fost negative pentru afec iuni renale. Examenul zic
eritrocite şi câteva leucocite. Osmolaritatea urinei a fost
a relevat o pacientă febrilă, cu stare generală modi cată,
381 mOsm/kg, sodiul 84,5 mEq/l, potasiu 22,3 mEq/l,
puls
92 bătăi pe minut, tensiune arterială
158/72
clor 78 mEq/l; proteinuria pe 24 de ore a fost 6800 mg.
mmHg (hipertensiune uşoară) şi edeme bilaterale ale
Datorită distensiei abdominale progresive şi ale
gleznelor cu godeu (+3) care se extindeau proximal până
acuzelor pacientei, respectiv dureri abdominale severe în
la mijlocul gambei. Nu a fost eviden iată nicio
cadranul inferior stâng, a fost trimisă pentru tomogra e
organomegalie, deşi a fost detectată o ascită uşoară până
computerizată (fără mediu de contrast). A fost observată
la moderată. Examinările cardiovasculare, respiratorii şi
o efuziune peritoneală masivă în abdomen şi pelvis, cu
neurologice nu au eviden iat modi cări semni cative.
mărirea nodulilor limfatici (până la 3,5 cm) în pelvis şi
Radiogra a toracică nu a arătat nicio patologie evidentă
limfadenopatie retroperitoneală şi inghinală bilaterală
(Figura 1).
(Figura 2).
Punc ia abdominală ulterioară, sub anestezie locală,
a relevat un lichid peritoneal lăptos. Examinările de
laborator au eviden iat trigliceride 126 mg/dl, colesterol
17 mg/dl, albumină 0,3 g/dl, glucoză 129 mg/dl, lactat
dehidrogenaza (LDH) 71 U/L, stabilind diagnosticul de
chiloperitoneu. Nu a fost găsită nicio dovadă de celule
tumorale la investiga iile citologice.
Evaluarea ginecologică nu a eviden iat dovezi de
malignitate sau alte patologii. Investiga iile osoase nu au
fost sugestive pentru mielom. Examinările de laborator
ulterioare au eviden iat următoarele constatări: Ac
hepatita C - nonreactiv, Ag hepatita B - nonreactiv,
Figura 1. Radiogra a toracică nu a arătat
nicio patologie evidentă la internare
sânge ocult în scaun - pozitiv, complement C3 - 58,2
A
B
C
Figura 2. CT abdominală arată o efuziune masivă peritoneală şi o mărire a nodulilor limfatici în cavitatea peritoneală,
pelvis, retroperitoneu şi spa iile inghinale bilaterale
110
Solun et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
mg/dl (interval normal 86-184 mg/dl), complement C4
Tratamentul combinat a fost început cu rituximab
- 11,2 mg/dl (interval normal 20-59 mg/dl), lan uri
(Rituxan®, Genentech Inc., San Francisco, CA) 375 mg/
uşoare libere kappa 20,2 mg/dl (interval normal 0,14-
m2 la ecare
3 săptămâni, dexametazonă (DexPak®,
2,42 mg/dl), lan uri uşoare libere lambda 6,98 mg/dl
Mikart Inc., Atlanta, GA)
40 mg o dată pe zi şi
(limite normale 0,02-0,67 mg/dl), imunoglobulina G
clorambucil
(Leukeran®, GlaxoSmithKline LLC,
(IgG) 433 mg% (interval normal 600-1600 mg%),
Philadelphia, PA)
2 mg o dată la
2 zile. Nivelul
imunoglobulina A 64,6 mg% (interval normal 100-430
creatininei a scăzut treptat până la
1,5 mg/dl, iar
mg%), imunoglobulina M 22,2 mg% (interval normal
proteinele urinare la 229 mg. Cu toate acestea, edemul
40-200 mg%). Testul crioglobulinelor serice a fost
membrelor inferioare şi ascita au rămas în mare parte
pozitiv. Biopsia medulară a demonstrat răspândirea
neschimbate.
difuză a unui număr mare de limfocite mici, consistente
După 4 cure de terapie a apărut febra, cu dispnee
cu diagnosticul de LLC (Fig. 3). Biopsia renală arătat un
progresivă. Pacienta a fost internată într-un alt spital, cu
model de MPGN, cu un singur tromb şi leziuni
pneumonie severă complicată cu un abces pulmonar şi
exudative focale. Colora ia prin imuno uorescen a
empiem pleural. În ciuda drenajului cavită ii
directă a eviden iat prezen a IgG. La microscopia
empiemului şi terapiei intensive cu antibiotice, starea
electronică s-au observat depuneri subendoteliale, cu un
pacientei a continuat să se deterioreze, decedând prin
model microtubular măsurând aproximativ
30
insu cien ă respiratorie şi cardiacă la 4 luni de la debutul
nanometri, consistent cu crioglobulina (Figura 4).
tratamentului.
A
B
Celule B pozitive la CD20 (× 20)
Celule B pozitive la colorarea membranei
cu CD5 (× 20)
C
D
Celule T proliferative pozitive la CD3 (× 20)
In ltrarea măduvei osoase cu celule
limfocitare mici (colora ie HE× 20)
Figura 3. Determinările biopsiei de măduvă osoasă. (A) Celule B pozitive la CD20 (× 20).
(B) Celule B pozitive la colorarea membranei cu CD5(× 20). (C) Celule T proliferative pozitive
la CD3 (× 20). (D) In ltrarea măduvei osoase cu celule limfocitare mici (colora ie HE× 20)
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
111
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
A
B
Necroză brinoidă prezentă într-o arteriolă
Glomerulonefrită cu model
mică (× 100)
membranoproliferativ prezentând un singur
tromb şi leziuni exudative focale (× 100 )
C
D
Colora ie prin imuno uorescen ă directă a
Microscopie electronică arătând depozite
IgG (× 200)
subendoteliale cu model microtubular
măsurând aproximativ 30 nanometri,
consistente cu crioglobulina
Figura 4. Biopsie renală. (A) Necroză brinoidă prezentă într-o arteriolă mică (mărire × 100);
(B) Glomerulonefrită cu model membranoproliferativ prezentând un singur tromb şi leziuni
exudative focale (mărire × 100), (C) Colora ie prin imuno uorescen ă directă a IgG (mărire ×
200), (D) Imagine de microscopie electronică arătând depozite subendoteliale cu model
microtubular măsurând aproximativ 30 nanometri, consistente cu crioglobulina
Discuție
glomerulare care pot înso i LLC [1]. Celelalte includ
glomerulonefrita semilunară, boala depunerii lan urilor
LLC este cel mai frecvent tip de leucemie la
uşoare, amiloidoza şi glomeruloscleroza focal
persoanele în vârstă în ările occidentale şi reprezintă
segmentară. MPGN poate cauzată de crioglobulinemie,
30% din totalul leucemiilor în Statele Unite ale Americii
predominant de tip I, eventual asociată cu depozite
[7]. Leziunea renală la pacien ii cu LLC este de obicei
organizate subendoteliale sau mezangiale şi trombi
asociată cu in ltrarea leucemică directă şi este un
proteici cu organizare microtubulară. Crioglobulinemia
eveniment comun. Cu toate acestea, implicarea
cristalină este caracterizată prin substructuri cristaline
glomerulară care duce la proteinurie de diferite severită i
foarte bine organizate care afectează diferite organe, în
şi sindrom nefrotic este extrem de rară. De obicei, este o
special rinichii şi sinoviala [9,10].
consecin ă a in ltrării difuze a tubilor renali şi
Crioglobulinemia este caracterizată prin prezen a de
comprimării microcircula iei, ducând la obstruc ia
proteine
anormale
sangvine
(în
principal
intrarenală şi ischemie
[2,8]. MPGN este cea mai
imunoglobuline), care se solidi că şi precipită la
comună formă dintre diferitele tipuri de patologii
temperaturi corporale reduse. În 1933, Wintrobe şi Buell
112
Solun et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
[11] au fost primii care au descris
„globulina serică
Klebsiella pneumoniae sunt responsabili pentru bacteriemie
precipitabilă la rece”, la un pacient cu semne şi simptome
şi septicemie la pacien ii cu neutropenie indusă de
de hipervâscozitate asociate unui mielom multiplu.
chimioterapie, asociată cu imunode cien a sus inută şi
Termenul a fost schimbat în crioglobulină de către
profundă a celulelor T [24,25]. Supresia imună celulară
Lerner şi Watson [12] în 1947. Conform clasi cării
poate duce de asemenea la infec ii cu germeni oportunişti,
clasice Brouet, crioglobulinemiile pot împăr ite în trei
cum ar Pneumocystis, Listeria, Nocardia, Mycobacterium,
grupe în func ie de tipul de anticorp produs [13]. Tipul I
virusurile herpetice, Candida şi Aspergillus [26,27]. Cea mai
(crioglobulinemia simplă) este în principal rezultatul
frecventă localizare a infec iei este tractul respirator
unui singur IgM monoclonal, deşi au fost raportate şi
(pneumonie severă avansată), urmată de tractul urinar,
IgG, IgA şi lan uri uşoare de imunoglobuline
[14].
piele şi esuturile moi. Într-un studiu retrospectiv pe 402
Aceasta este de obicei asociată cu tulburări
de pacien i cu LLC trata i cu udarabină ca monoterapie
limfoproliferative cum ar mielomul multiplu, LLC şi
sau în combina ie cu corticosteroizi, Anaissie şi colab. [28]
macroglobulinemia Waldenstrom. Tipul II con ine
au remarcat o rată de 58% de infec ii majore la pacien ii
factor reumatoid monoclonal, de obicei IgM şi o
trata i anterior, comparativ cu 34% la pacien ii netrata i
componentă policlonală. Tipul III con ine componente
anterior. La analiza multivariată, factorii semni cativi şi
policlonale IgG şi IgM. Tipurile II şi III sunt men ionate
independen i de risc pentru infec ie au fost stadiul avansat
de asemenea ca crioglobulinemii mixte şi reprezintă 80%
al bolii (Rai III şi IV), istoricul de chimioterapie anterioară
din toate cazurile de crioglobulinemie. Ele sunt mai des
(sau răspunsul slab), nivelul crescut al creatininei serice,
întâlnite la pacien ii cu infec ii cronice şi boli autoimune.
nivelul scăzut al albuminei serice şi scăderea numărului de
Cei mai mul i pacien i cu crioglobulinemie mixtă au
granulocite.
infec ie cronică cu virusul hepatitei C [15,16,17].
Tipul I de crioglobulinemie este caracterizat prin
Concluzie
leziuni în zonele independente (cap şi mucoasă) şi se
manifestă sub formă de fenomen Raynaud, livedo
Descriem cazul unei paciente cu LLC complicată
reticularis şi ulcera ii
[18,19]. Manifestări musculo-
prin insu cien ă renală acută, sindrom nefrotic şi
scheletale apar la 35%-72% din cazuri, cel mai adesea în
crioglobulinemie. Deşi implicarea renală datorată direct
tipurile II şi III. Bolile renale, raportate la 5% până la
in ltrării leucemice este relativ frecventă la pacien ii cu
60% dintre pacien ii cu crioglobulinemie precum şi
LLC, insu cien a renală acută cu sindrom nefrotic şi
neuropatie, raportate la 10% la 80%, sunt de asemenea,
crioglobulinemie este extrem de rară. MPGN este cea
de obicei, asociate cu tipurile mixte. Manifestările mai
mai frecventă patologie glomerulară la pacien ii cu LLC.
pu in frecvente includ dureri abdominale (2%-22%),
Tratamentul cu clorambucil, prednisolon şi anticorpi
acrocianoza (9%) şi tromboza arterială (1%). Implicarea
monoclonali stabilizează func ia renală. Infec ia este un
renală este una dintre cele mai grave complica ii ale
factor de risc major în evolu ia clinică a LLC şi cauza
crioglobulinemiei. Aceasta apare de obicei în termen de
principală de morbiditate şi mortalitate. Patogeneza
3-5 ani de la diagnostic, cu o prevalen ă mai mare în
infec iei în acest context este multifactorială şi de obicei
crioglobulinemia mixtă [17,20,21]. Din punct de vedere
asociată hipogammaglobulinemiei şi tratamentului cu
clinic, cele mai comune caracteristici ale afectării renale
anticorpi monoclonali şi imunosupresoare. La pacienta
sunt proteinuria izolată şi hematuria, e microscopică,
noastră, func ia renală s-a ameliorat după tratamentul
e macroscopică, urmate de sindrom nefritic/nefrotic şi
cu rituximab, dexametazonă şi clorambucil, dar ea a
insu cien ă renală acută [22].
decedat câteva luni mai târziu prin complica iile severe
Pacien ii cu LLC sunt predispuşi la complica ii
ale unei pneumonii.
infec ioase, care sunt principala cauză de morbiditate şi
mortalitate legată de LLC, studiile arătând că infec iile
sunt responsabile pentru 30% până la 50% din totalul
Referințe
deceselor [23]. Susceptibilitatea la infec ii este asociată cu
hipogammaglobulinemie şi ulterior imunosupresie
1. Favr Favre G, Courtellemont C, Callard P, et al.
secundară tratamentului cu steroizi, imunosupresoare şi
Membranoproliferative glomerulonephritis, chronic
anticorpi monoclonali. Cele mai multe dintre infec ii sunt
lymphocytic leukemia, and cryoglobulinemia. Am J
la origine bacteriene, principalele vinovate ind bacteriile
Kidney Dis 2010 ;55(2) :391-4.
încapsulate, cum ar
Streptococcus pneumoniae şi
2. Dou X, Hu H, Ju Y, et al. Concurrent nephrotic
Haemophilus in uenzae. Germenii patogeni gram-negativi,
syndrome and acute renal failure caused by chronic
cum ar
Pseudomonas aeruginosa, Escherichia coli,
lymphocytic leukemia (CLL): a case report and literature
Nephrotic Syndrome and Acute Renal Failure Caused by Chronic Lymphocytic Leukemia
113
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
review. Diagn Pathol 2011 ;6 :99. Doi : 10.1186/1746-
16.
Sansonno D, Dammacco F. Hepatitis C virus,
1596-6-99.
cryoglobulinaemia, and vasculitis
: immune complex
3.
Mutluay R, Aki SZ, Erten Y, et al.
relations. Lancet Infect Dis 2005 ;5 :227.
Membranoproliferative glomerulonephritis and light-
17.
Sene D, Ghillani-Dalbin P, ibault V, et al. Long-term
chain nephropathy in association with chronic
course of mixed cryoglobulinemia in patients infected with
lymphocytic leukemia. Clin Nephrol 2008 ;70(6) :527-
hepatitis C virus. J Rheumatol 2004;31:2199-206.
31.
18.
Monti G, Galli M, Invernizzi F, et al.
4.
Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann
Cryoglobulinaemias: a multi-centre study of the early
M. Biologic and clinical signi cance of cryoglobulins. A
clinical and laboratory manifestations of primary and
report of 86 cases. Am J Med 1974;57(5):775-88.
secondary disease. GISC. Italian Group for the Study
5.
Aslam N, Nseir NI, Viverett JF, Bastacky SI, Johnson
of Cryoglobulinaemias. QJM 1995;88(2):115-26.
JP. Nephrotic syndrome in chronic lymphocytic leukemia:
19.
Rossi D, Mansouri M, Baldovino S, et al. Nail fold
a
paraneoplastic
syndrome?
Clin
Nephrol
videocapillaroscopy in mixed cryoglobulinaemia.
2000;54(6):492-7.
Nephrol Dial Transplant 2004;19(9):2245-9.
6.
Moulin B, Ronco PM, Mougenot B, Francois A,
20.
Ferri C, La Civita L, Cira si C, et al. Peripheral
Fillastre JP, Mignon F. Glomerulonephritis in chronic
neuropathy in mixed cryoglobulinemia: clinical and
lymphocytic leukemia and related B-cell lymphomas.
electrophysiologic
investigations.
J
Rheumatol
Kidney Int 1992;42(1):127-35.
1992;19(6):889-95.
7.
Siegel R, Naishadham D, Jemal A. Cancer statistics,
21.
Satish S, Rajesh R, George K, Elango EM, Unni VN.
2012. CA Cancer J Clin 2012;62(1):10.
Membranoproliferative glomerulonephritis with essential
8.
Rifkin SI. Acute renal failure secondary to chronic
cryoglobulinemia. Indian J Nephrol 2008;18(2):80-2.
lymphocytic leukemia: a casereport. Medscape J Med
22.
Alchi
B,
Jayne
D. Membranoproliferative
2008;10(3):67.
glomerulonephritis. Pediatr Nephrol 2010;25(8):1409-
9.
Galea HR, Bridoux F, Aldigier JC, et al. Molecular
18.
study of an IgG1kappa Cryoglobulin yielding organized
23.
Francis S, Karanth M, Pratt G, et al. e e ect of
microtubular deposits and glomerulonephritis in the
immunoglobulin VH gene mutation status and other
course of chronic lymphocytic leukaemia. Clin Exp
prognostic factors on the incidence of major infections in
Immunol 2002 ;129(1) :113-8.
patients with chronic lymphocytic leukemia. Cancer
10.
Papo T, Musset L, Bardin T, et al.
2006;107(5):1023-33.
Cryocrystalglobulinaemia as a cause of systemic
24.
Morrison VA. Infectious complications in patients with
vasculopathy and widespread erosive arthropathy.
chronic lymphocytic leukemia: pathogenesis, spectrum of
Arthritis Rheum 1996;39:335-40.
infection, and approaches to prophylaxis. Clin
11.
Wintrobe MM, Buell MV. Hyperproteinemia
Lymphoma Myeloma 2009;9(5):365-70.
associated with multiple myeloma: with report of a case
25.
Nosari A. Infectious Complications in Chronic
in which an extraordinary hyperproteinemia was
Lymphocytic Leukemia. Mediterr J Hematol Infect Dis
associated with thrombosis of the retinal veins and
2012;4(1):e2012070. Epub
2012 Nov
5. doi:
symptoms suggesting Reynaud’s disease. Bull Johns
10.4084/MJHID.2012.070.
Hopkins Hosp 1933;52:156.
26.
Byrd JC, Hargis JB, Kester KE, Hospenthal DR,
12.
Lerner AB, Watson CJ. Studies of cryoglobulins;
Knutson SW, Diehl LF. Opportunistic pulmonary
unusual purpura associated with the presence of a high
infections with udarabine in previously treated patients
concentration of cryoglobulin (cold precipitable serum
with low-grade lymphoid malignancies: A role for
globulin). Am J Med Sci 1947;214(4):410.
Pneumocystis carinii pneumonia prophylaxis. Am J
13.
Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann
Hematol 1995;49(2):135-42.
M. Biologic and clinical signi cance of cryoglobulins: a
27.
Morrison VA. Infectious complications of chronic
report of 86 cases. Am J Med 1974;57:775.
lymphocytic leukaemia: pathogenesis, spectrum of
14.
Morra E. Cryoglobulinemia. Hematology Am Soc
infection, preventive approaches. Best Pract Res Clin
Hematol Educ Program 2005:368-72.
Haematol 2010;23(1):145-53.
15.
Cacoub P, Costedoat-Chalumeau N, Lidove O, Alric
28. Anaissie EJ, Kontoyiannis DP, O’Brien S, et al. Infections
L. Cryoglobulinemia vasculitis. Curr Opin Rheumatol
in patients with chronic lymphocytic leukemia treated with
2002;14(1):29-35.
udarabine. Ann Intern Med 1998;129(7):559-66.
Traducere: dr Călin Bumbulu
114
Solun et al
CASE PRESENTATION
LITIAZĂ VEZICALĂ SECUNDARĂ UNUI DISPOZITIV INTRAUTERIN
MIGRAT. PREZENTARE DE CAZ
Victor Ona1, Bogdan Feciche2, Andrei Boc1, Dan Ona3, Ioan Coman1
1Clinica de Urologie, Spitalul Clinic Municipal Cluj-Napoca, 2Spitalul Judetean de Urgen ă Satu Mare şi 3Clinica de
Obstetrică şi Ginecologie I Cluj-Napoca, România
Adresa pentru coresponden ă:
Ona Victor MD PhD FEBU
E-mail: ona_victor@yahoo.de
Primit: 19.12.2013
Acceptat: 23.02.2014
Med Con March 2014, Vol 9, No 1, 115-118
Rezumat
rar şi care se poate complica cu dezvoltarea de calculi la
acest nivel.
Deşi sunt folosite ca metode e ciente de contracep ie
Prezentăm cazul unei paciente de 64 de ani cu această
de mai bine de 30 de ani, dispozitivele de contracep ie
patologie,
ind subliniate aspecte diagnostice,
intrauterină
(DIU) nu sunt lipsite de complica ii.
predispozante şi ale rezolvării chirurgicale minim invazive.
Migrarea este una dintre complica iile cunoscute ale
DIU.
Prezentare de caz
Prezentăm cazul unei paciente în varstă de 64 de ani
diagnosticată cu litiază vezicală secundară migrarii
În cadrul Sec iei de Urologie a Spitalului Clinic
intravezicale a unui dispozitiv intrauterin implantat în
Municipal Cluj-Napoca se prezintă în ambulator o
urmă cu 20 de ani. Sunt expuse metodele prin care s-a
pacientă în vârstă de
64 ani, acuzând hematurie
ajuns la stabilirea diagnosticului, precum şi rezolvarea
intermitentă, dureri pelvine nesistematizate, polakiurie
minim invazivă a acestei complica ii.
şi disurie. Pacienta fusese dirijată dintr-un alt serviciu
Cuvinte cheie: dispozitive de contracep ie
medical cu suspiciunea clinică şi ultrasonogra că de
intrauterină, litiază vezicală, chirurgie endoscopică
tumoră vezicală calci cată. Din antecedente re inem o
naştere prin opera ie cezariană efectuată în urmă cu 38
Introducere
ani şi menopauza naturală cu debut precoce, în jurul
vârstei de 44 ani. Examenul de urină arată hematurie
Dispozitivele de contracep ie intrauterină
(DIU)
microscopică 12 Ery/µl, uşoară leucociturie 20 Leu/µl
sunt folosite de mai bine de 30 de ani [1]. Deşi cunoscute
cu nitri i negativi. Ecogra a abdominală descrie un uter
ca ind metode e ciente şi sigure de cotracep ie, uneori
atro c şi eviden iază o forma iune hiperecogenă cu un
aceste dispozitive generează complica ii cu un impact
con de umbră posterior localizată la nivelul domului
important asupra pacientei, precum: perfora ii uterine,
vezicii, sugerând o imagine de calcul vezical suspendat.
abcese pelvine sau şoc septic. Inciden a perfora iei
În vecinătatea calculului s-a eviden iat o structură
uterine cauzată de DIU este scăzută. Totuşi în literatură
hiperecogenă în forma literei T, iar cavitatea uterină era
sunt publicate în jur de
100 de cazuri de migrare
de aspect normal, corespunzator vârstei menopauzale de
extrauterină a acestor dispozitive [2].
aproximativ 20 de ani. Examenul radiogra c abdominal
Migrarea tardivă intravezicală a dispozitivelor
simplu a arătat în aria de proiec ie a vezicii urinare o
intrauterine (DIU) reprezintă un eveniment extrem de
imagine radioopacă sugestivă pentru litiază, care
Bladder Lithiasis Secondary to a Migrated Intrauterine Device. Case Report
115
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
A
B
Figura 1. Radiogra a de bazin prezintă în aria de proiec ie a vezicii urinare o forma iune
calcară ataşată de un dispozitiv intrauterin a at în pozi ie ne ziologică (A), dispozitiv
intrauterin, detaliu (B)
Figura 2. Aspectul endoscopic al litiazei
dezvoltate pe sterilet migrat intravezical
Figura 3. Efectuarea litotri iei cu energie LASER Holmium prin dispozitiv inserat
pe canalul lucrativ al cistoscopului
prezenta ataşat un dispozitiv intrauterin a at în pozi ie
Ini ial s-a realizat litotri ia şi ulterior s-a efectuat incizia
anatomică anormală, Figura 1.
lineară a mucoasei vezicale suprajacente bra ului DIU
Reluând anamneza, pacienta con rmă că la
(Figura 3).
începutul anilor ’90 i s-a montat un sterilet şi că nu a
Extragerea steriletului cu ajutorul pensei extractoare
mai efectuat control ginecologic până în prezent. S-a
endoscopice, mucoasa prezentând o minimă hemoragie
practicat uretrocistoscopie şi s-a stabilit diagnosticul de
punctiformă este ilustrată în Figura
4. La sfârşitul
litiază vezicală dezvoltată pe dispozitiv intrauterin
interven iei s-a montat sondă uretro-vezicală Foley 16
migrat par ial intravezical. În Figura
2 se observă
Ch.
aspectul cistoscopic al vezicii urinare.
Postoperator evolu ia a fost favorabilă, cu externare
S-a decis şi s-a practicat în anestezie spinală litotri ie
după 48h, iar sonda uretro-vezicală s-a suprimat la 14
vezicală endoscopică cu dispozitiv LASER Holmium. zile. Evaluarea efectuată la 3 luni postoperator a relevat
116
Ona et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
CASE PRESENTATION
Figura 4. Steriletul extras endoscopic
Figura 5. Aspectul endoscopic al peretelui
vezical la cistoscopia de control la 3 luni
postoperator demonstrează vindecarea optimă
un status optimal din punct de vedere bacteriologic,
omentului în 23 cazuri, rectosigmoidului 44, peritoneului
ecogra c şi cistoscopic (Figura 5).
41, vezicii urinare 23, apendicelui 8, intestinului sub ire
2, anexei 1 şi respectiv venei iliace un caz.
Discuții
Majoritatea autorilor recomandă îndepărtarea
dispozitivelor intrauterine con inând cupru datorită
Cazul nostru este particular prin raritatea sa,
poten ialului de reac ii in amatorii care pot cauza ocluzie
datorită perioadei îndelungate de la montarea DIU la
sau perfora ie intestinală. În plus există motive pentru
diagnosticul şi tratamentul complica iei.
îndepărtarea tuturor dispozitivelor intrauterine migrate,
La cazul mai sus men ionat a existat un interval
precum compromiterea func ională a structurilor
liber între aplicarea steriletului şi apari ia manifestărilor
adiacente, infec ia şi anxietatea pacientei după stabilirea
urinare ce au implicat explorări paraclinice soldate cu
diagnosticului de corp străin intra-abdominal [4].
surpriza eviden ierii intravezicale a corpului străin
Deşi laparoscopia este preferată explorării
migrat, care a suportat apoi depuneri minerale şi au dus
chirurgicale clasice, trebuie totuşi inut cont de
ini ial la confuzia cu o tumoră vezicală calci cată.
posibilitatea conversiei datorită di cultă ilor întâlnite în
Considerăm că experien a limitată în aplicarea
cazul acestor interven ii [3].
steriletului la data montării acestuia a fost factorul
Între anii
1999-2009 în literatură au mai fost
decisiv în apari ia complica iilor tardive.
comunicate încă 9 cazuri de litiază vezicală secundară
Aportul chirurgiei minim invazive endoscopice este
unui dispozitiv intrauterin migrat [1,2,5-10].
fundamental, iar evolu ia favorabilă este o consecin ă a
Se consideră că producerea unei zone de continuitate
tenhicii chirurgicale care respectă continuitatea uroteliului.
la nivel uterin are loc sau debutează cu ocazia inser iei lui,
Migrarea intra-abdominală a unui dispozitiv de
riscul ind de 2,2 cazuri la 1000 de aplicări [11]. Aplicarea
contracep ie intrauterină este rară. Kassak şi Audra [3],
corectă a unui DIU implică respectarea unor indica ii şi
într-o revistă a literaturii pe o perioadă de 18 ani, au
contraindica ii, unele absolute, altele relative. Existen a
raportat un număr de 165 de cazuri de migrare intra-
unei cicatrici uterine, consecin a unei naşteri prin sec iune
abdominală a IUCD. Acestea au fost localizate la nivelul
cezariană, măreşte riscul unui accident soldat cu perforarea
Bladder Lithiasis Secondary to a Migrated Intrauterine Device. Case Report
117
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
completă sau par ială a uterului la nivelul unei zone de
4.
Ozgun MT, Batukan C, Serin IS, Ozcelik B, Basbug
rezisten ă mai mică. De obicei perforarea uterului datorită
M, Dolanbay M. Surgical management of intra-
unor condi ii anatomice locale se produce la nivelul zonei
abdominal
mislocated
intrauterine
devices.
fundice, nerecunoaşterea imediată a acestui accident
Contraception 2007;75(2):96-100.
putându-se rezolva celioscopic. În unele cazuri, prezen a
5.
Insausti Jaca N, Urresola Olabarrieta A, Ibáñez S, et
raporturilor de vecinatate anatomică cu plica vezico-
al. Uterovesical perforation secondary to intrauterine
uterină, destinsă în deple ie, alături de existen a unei zone
device with vesical lithiasis formation: a report of two
de alterare histologică a miometrului creată de incizia
cases. Radiologia 2007;49(2):129-32.
segmentară de la o sec iune cezariană, realizează o cauză
6.
Singh I. Intravesical Cu-T emigration: an atypical and
iritativă locală manifestată prin menometroragii trenante,
infrequent cause of vesical calculus. Int Urol Nephrol
sau prin posibilitatea migrării complete sau par iale a
2007;39(2):457-9.
steriletului în vezica urinară.
7.
Hick EJ, Hernández J, Yordán R, Morey AF, Avilés R,
În concluzie, litiaza vezicală dezvoltată pe DIU
García CR. Bladder calculus resulting from the
migrat intravezical reprezintă o situa ie clinică rară, dar
migration of an intrauterine contraceptive device. J Urol
nu imposibil de întâlnit în practică. Rezolvarea minim
2004;172(5 Pt 1):1903.
invazivă utilizând arsenalul chirurgiei endoscopice este
8.
Iturralde Codina A, Gozá León F, Beyríes Tamayo W,
posibilă, iar evolu ia postoperatorie este optimă.
Iturralde Muñoz Y, Rodríguez Hidalgo ME. Double
bladder lithiasis from an intrauterine device. Report one
case. Arch Esp Urol 2004;57(2):160-2.
Referințe
9.
Ozçelik B, Serin IS, Basbug M, Aygen E, Ekmekçioglu
O. Di erential diagnosis of intra-uterine device
1. Mustafa M. Erosion of an intrauterine contraceptive
migrating to bladder using radiographic image of
device through the bladder wall causing calculus:
calculus formation and review of literature. Eur J Obstet
management and review of the literature. Urol Int
Gynecol Reprod Biol 2003;108(1):94-6.
2009;82(3):370-1.
10.
Nouri M, Fassi M, Koutani A, Ibn Attya A, Hachimi
2. Ozgür A, Sişmanoğlu A, Yazici C, Coşar E, Tezen D,
M, Lakrissa A. Migration of an intrauterine device into
Ilker Y. Intravesical stone formation on intrauterine
the bladder. Report of a case. J Gynecol Obstet Biol
contraceptive device. Int Urol Nephrol 2004;36(3):345-
Reprod (Paris) 1999;28(2):162-4.
8.
11.
E. Caliskan, N. Ozturk, B.O. Dilbaz, S. Dilbaz.
3. Kassab B, Audra P. e migrating intrauterine device.
Analysis of risk factors associated with uterine perforation
Case report and review of the literature. Contracept
by intrauterine devices. Eur J Contracept Reprod
Fertil Sex 1999;27(10):696-700.
Health Care 2003;8(3):150-5.
118
Ona et al
MEDICINE AND ART
PICTURILE REPREZENTÂND UN CAZ DE OBEZITATE DIN SECOLUL
AL XVII LEA, DATORAT PROBABIL SINDROMULUI PRADER WILLI
Călin Bumbulu1, Andrei Bumbulu2, Alina Daniela Negru1, Rumelia Koren3
1SCM dr Bumbulu - dr Balaj, Satu Mare, România, 2Facultatea de Medicină, Universitatea de Medicină şi Farmacie
Iuliu Ha ieganu, Cluj Napoca, România, 3Departmentul de Patologie, Spitalul Hasharon, Petah Tikva şi Facultatea de
Medicină Sackler, Universitatea Tel-Aviv, Israel
Adresa pentru coresponden ă:
Dr. Bumbulu Călin
Satu Mare, str. Bobocului UK 30-440258
E-mail: bumbulutcalin@yahoo.com
Primit: 06.10.2013
Acceptat: 10.12.2013
Med Con March 2014, Vol 9, No 1, 119-121
Rezumat
Într-o analiză sistematică a unor portrete descriind
semne vizibile de boală [2] pe o colec ie de picturi
De-a lungul Evului Mediu și a Renașterii obezitatea
reprezentând
3.615 de locuitori ai unei regiuni
a fost adesea văzută ca un semn al bogă iei. Acum știm
geogra ce determinate, acoperind mai multe secole,
că excesul ponderal și obezitatea sunt dăunătoare
excesul de greutate a fost mai frecvent la bărba i decât la
sănătă ii, iar prevenirea obezită ii este o intă a sănătă ii
femei (30% vs. 44%). Excesul de greutate a fost cel mai
publice. Prezentăm două portrete ale Eugeniei Martínez
frecvent la cei de peste 40 de ani fa ă de cei cu vârsta sub
Vallejo, o feti ă de 8 ani supranumită „Monstrul” din
40 de ani. Alte condi ii, cum ar membre amputate,
cauza obezită ii ei, cauzată probabil de sindromul
lipsa din ilor, sau deformările date de osteoartrită au fost
Prader-Willi, pictate de unul dintre pictorii de curte cei
surprinzator de rar descrise în portretele evaluate.
mai respecta i ai secolului al XVII-lea, Juan Carreño de
Asocierea dintre excesul de greutate și vârsta mai
Miranda.
înaintată a fost mai pronun ată în picturile din secolele
Cuvinte cheie: sindrom Prader-Willi, obezitate,
XVII și XVIII. În secolul al XVIII-lea, în rândul
pictură, Juan Carreño de Miranda
oamenilor de peste 40 de ani, 79% dintre bărba i au fost
supraponderali, comparativ cu 51% dintre femei. Din
Imaginea pe care ecare dintre noi o avem despre
secolul al XVIII-lea până în secolul al XX-lea prevalen a
propriul nostru corp afectează profund felul în care ne
supraponderalită ii a scăzut la barba ii de peste 40 de
rela ionăm cu societatea. Reprezentările obezită ii în
ani.
artă oferă un context pentru o re ectare asupra
În Figura 1 este un exemplu al gustului baroc pentru
schimbărilor pe care obezitatea o determină asupra
reprezentările anomaliilor naturii și al atrac iei oamenilor
indivizilor și societă ii. De-a lungul Evului Mediu și a
fa ă de unele anomalii zice sau psihologice. În această
Renașterii obezitatea a fost adesea văzută ca un semn al
pictură ia forma prezentării unei feti e cu dimensiuni
bogă iei, ind relativ comună în rândul elitei societă ii
extraordinare, posibil datorate sindromului Prader-Willi
[1]. Desigur, știm acum că excesul de greutate și
[3]. Plasarea modelului pe un fundal neutru urmează
obezitatea sunt dăunătoare sănătă ii, iar prevenirea
tradi iei portretisticii de la Curtea spaniolă. Eugenia
obezită ii este un obiectiv al sănătă ii publice.
Martínez Vallejo a fost introdusă la Curtea regală în
Paintings of a Case of Obesity in the 17th Century, Probably Due to Prader-Willi Syndrome
119
MEDICINE AND ART
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Figura 1. Juan Carreño de Miranda, “Eugenia Martínez Vallejo, La monstrua vestida”, ulei pe pânza,
Madrid, Museo del Prado, 1680
Figura 2. Eugenia Martínez Vallejo, sculptură
de Amado González Hevia, Aviles, Spania
120
Bumbuluț et al
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
MEDICINE AND ART
1680, iar portretul ei a fost pictat din ordinul direct al
afectează sexul masculin sau feminin cu o frecven ă
regelui Carlos al II-lea. A fost una dintre persoanele cu
egală, implicând toate rasele și etniile.
defecte zice sau psihice care au format o mică Curte în
Se spune că văzând pictura din Muzeul Prado, Dr.
jurul moștenitorilor coroanei spaniole.
Andrea Prader a recunoscut imediat caracteristicile ca
Copilul de 8 ani a fost numit „Monstrul” din cauza
ind concordante cu sindromul Prader-Willi. Deși
obezită ii. Există și o altă pictură a Eugeniei, dezbrăcată,
poate niciodată nu vom ști dacă acest copil a avut de
ambele picturi a ându-se la Muzeul Prado. Deformitatea
fapt PWS, pictura și descrierea simptomelor sale sprijină
ei este accentuată de minunata rochie roșie în orată,
puternic această ipoteză. Acest tablou este adesea
care drapează corpul imens. Culoarea rochiei face ca
considerat ca ind cea mai veche ilustrare a PWS. La
nuditatea din portretul alăturat să e mai explicită.
Monstrua a continuat să e de-a lungul istoriei o gură
Eugenia Martínez Vallejo a fost expusă mul imilor
interesantă, fapt demonstrat și de o sculptură în aer liber
la diferite târguri. Rolul jucat de aceste persoane la Curte
din Aviles, creată în
1997 de către artistul spaniol
a fost de multe ori foarte important. Ele au oferit
Amado González Hevia și care s-a bazat pe portretele
companie multor prin i și prin ese și deoarece înăl imea
Eugeniei făcute de Juan Carreño de Miranda (Figura 2).
lor era similară cu cea a copiilor, Infan ii se sim eau
Originea maternă a materialului genetic care este
confortabil în preajma lor. În plus, vârsta acestora
afectat în sindrom este importantă, deoarece regiunea
însemna că urmașii regali aveau un con dent permanent
speci că implicată a cromozomului
15, una dintre
care le asigura întotdeauna îngrijirea, precum și
regiunile cele mai complexe din genomul uman, este
divertismentul necesar. Atunci când creșteau, deseori
supusă imprimării parentale de origine, ceea ce înseamnă
prin ii și prin esele ineau pe lângă ei pe acești prieteni
că pentru un număr de gene din această regiune doar o
din copilărie, cum a făcut și Isabela Clara, ica lui Philip
copie a genei este exprimată, în timp ce cealaltă este
al II-lea, adesea pictată împreună cu piticul ei, care a
represată în cursul imprimării. Pentru genele afectate în
plâns mai mult decât oricine atunci când ea a murit.
PWS, de obicei este imprimată copia maternă (și aceasta
Aceste portrete au fost pictate de către unul dintre
este represată), în timp ce copia mutantă paternă nu este
cei mai respecta i pictori ai Cur ii, Juan Carreño de
func ională. Acest lucru înseamnă că în timp ce
Miranda (25 martie 1614-3 octombrie 1685), care a
majoritatea oamenilor au o singură copie func ională a
folosit-o pe Eugenia de câteva ori ca model. Carreño a
acestor gene, persoanele cu PWS au o copie de
descris via a la Curtea lui Carlos al II-lea mai bine decât
nefunc ională și una represată. Dacă în schimb este
orice alt pictor, dezvăluind slăbiciunile regelui, care a
afectat materialul genetic matern din aceeași regiune,
ajuns să e cunoscut sub numele de „Cel Vrăjit”. El a
rezultatul este sindromul opus- sindromul Angelman.
refuzat să e numit cavaler al Ordinului de Santiago,
În zilele noastre, bene ciind de recentele progrese ale
spunând că „pictura nu are nevoie de onoruri, ea le poate
diagnosticului precoce și ale interven iilor terapeutice,
da întregii lumi”. Nobil prin origine, el a avut o în elegere
rata obezită ii în rândul copiilor cu sindrom Prader-Willi
a mecanismelor și a psihologiei Cur ii regale ca niciun
a scăzut până la a similară cu a popula iei generale.
pictor înainte, pictând portretele familiei regale spaniole
Sindroamele Angelman, Prader-Willi și duplica ia
într-un mod descriptiv fără precedent. Cele mai multe
cromozomului 15q sunt condi ii speci ce cauzate de diferite
dintre lucrările lui sunt portrete ale familiei regale și ale
variante genetice ale aceleaiași regiuni genetice. 15 noiembrie
Cur ii, deși există și câteva lucrări timpurii comandate în
a fost declarată Ziua Interna ională a 15q pentru a crește
principal de către biserică, piese de altar.
aten ia asupra similitudinilor dintre aceste sindroame.
Sindromul Prader-Willi
(PWS) este o afec iune
genetică rară, în care șapte gene de pe cromozomul 15
sunt deletate sau neexprimate
(dele ie par ială a
Referințe
cromozomului 15q) pe cromozomul patern. A fost
descris pentru prima dată în
1956 de către Andrea
1. Ferrucci L, Studenski SA, Alley DE, Barbagallo M,
Prader, Heinrich Willi, Alexis Labhart, Andrew Ziegler
Harris TB. Obesity in Aging and Art. J Gerontol A
și Guido Fanconi. Caracteristicile PWS sunt mâinile și
Biol Sci Med Sci 2010;65A(1):53-56.
picioarele mici, statura mică, tonusul muscular scăzut,
2. Als C, Stüssi Y, Boschung U, Tröhler U, Wäber JH.
dizabilită ile cognitive, problemele comportamentale,
Visible signs of illness from the 14th to the 20th century:
dezvoltarea sexuală incompletă și senza ia cronică de
systematic review of portraits. BMJ 2002;325(7378):1499.
foame care poate duce la mâncatul excesiv și la obezitate
3. Pozzilli P, Khazrai YM. „La Monstrua Vestida”, a case
amenin ătoare de via ă. Inciden a PWS este între unul
of Prader-Willi syndrome. J Endocrinol Invest
din 25.000 și unul din 10.000 de nou-născu i vii. PWS
2005;28(2):199.
Paintings of a Case of Obesity in the 17th Century, Probably Due to Prader-Willi Syndrome
121
ZILELE MEDICALE SĂTMĂRENE EDIȚIA A X-A, 16-18 octombrie 2014
PRIMUL ANUNȚ
Joi 16 Octombrie 2014
09:00 - 09:30
- Primirea participan ilor. Validarea participării. Înscrieri. Înmânarea documentelor manifestării.
09:30
- Deschiderea o cială
10:00 - 17:00
- Sesiune de comunicări lucrări ştiin i ce cu pauze: pentru cafea şi pentru prânz
Vineri 17 Octombrie 2014
09:00 - 16:00
- Sesiune de comunicări lucrări ştiin i ce cu pauze: pentru cafea şi pentru prânz
Sâmbătă 18 Octombrie 2014
09:00 - 16:00
- Sesiune de comunicări lucrări ştiin i ce şi Sec iunea de Istorie medicală sătmăreană cu pauze:
pentru cafea şi pentru prânz. Înmânarea certi catelor de participare. Înmânarea diplomelor de
excelen ă pe baza voturilor participan ilor.
INFORMA II GENERALE
Conferin ă regională, cu participare interna ională
Loca ie: Filarmonica Dinu Lipatti Satu Mare
Organizator: COLEGIUL MEDICILOR SATU MARE
Parteneri: ASOCIA IA MEDICILOR DE FAMILIE SATU MARE, CENTRUL MEDICAL RABIN-
UNIVERSITATEA TEL AVIV ISRAEL, UNIVERSITATEA
„TITU MAIORESCU” BUCUREŞTI,
UNIVERSITATEA DE VEST „VASILE GOLDIŞ” ARAD- FILIALA SATU MARE
Preşedintele Comitetului Ştiin i c: Prof. Univ. Dr. Rumelia Koren
ÎNSCRIERE
Pute i să vă înscrie i:
- personal la sediul Colegiului Medicilor Satu Mare
- prin poştă, pe adresa: Colegiul Medicilor Satu Mare, P- a Eroilor Revolu iei nr. 23, cod poştal 440055
- prin fax la numărul: 0361-408164, e-mail: colmedsm@gmail.com
Înregistrarea va validată doar după dovada plă ii taxei de participare.
TAXA DE PARTICIPARE
- Medici, specialişti, primari - 60 lei
Până la 31.08.2014
- Medici reziden i, studen i, pensionari - gratuit
- Medici, specialişti, primari - 70 lei
După 31.08. 2014 şi pe loc
- Medici reziden i, pensionari - 20 lei
- se poate plăti în contul Colegiului Medicilor Satu Mare: RO21BTRL03101205K39262XX, deschis la Banca
Transilvania Satu Mare, cu men ionarea: taxă participare 16-18.10.2014 şi numele participantului
- se poate achita direct la sediul Colegiului Medicilor Satu Mare
Taxa de participare include: mapa cu documentele manifestării, accesul la sesiunile de lucru, co ee-break-uri,
bufetul suedez pentru ecare zi.
Pentru rezervări cazare până la data de 30.09.2013: tel 0261-710456, e-mail: colmedsm@gmail.com
LUCRĂRI
Termenul pentru predare a rezumatelor este 1 septembrie 2013.
Comitetul ştiin i c îşi rezervă dreptul de a accepta sau respinge lucrările propuse.
Lucrările participan ilor vor sub formă de prezentare în format Power Point şi vor sus inute oral timp de 10 minute.
Termenul limită de predare a lucrărilor în format Power Point este 15 septembrie 2014.
LUCRĂRI IN EXTENSO
Lucrările in extenso vor publicate în revista „Conexiuni Medicale” nr. 4/2014, cu condi ia să e înaintate
la adresa de e-mail bumbulutcalin@yahoo.com.
Se acceptă doar lucrări nepublicate, autorii asumându-şi integral răspunderea con inutului.
122
GUIDANCE FOR DRAWING UP
STANDARDE DE REDACTARE
Scop
materiale care ar putea să îi identi ce. Dacă formularele
Revista Conexiuni Medicale publică lucrări de
de accept nu prevăd acest lucru vă rugăm să rugăm
cercetare care contribuie la progresul din toate domeniile
ob ine i acordul, sau îndepărta i posibilitatea de
medicinei. Revista publică de asemenea reviste generale,
identi care. O declara ie în acest sens trebuie inclusă în
editoriale și scurte comunicări pe domenii speci ce.
sec iunea „Metode” a lucrării.
Prezentările de caz sunt acceptate dacă prezintă interes
crescut și sunt bine investigate. Scrisorile către editor, în
Aprobarea Comitetului de Etică
special cele care prezintă o opinie privind un articol
Preciza i la sec iunea „Metode” faptul că desfășura i
publicat anterior sau care prezintă noi date, sunt de
studii asupra subiec ilor umani cu aprobarea Spitalului,
asemenea binevenite. Adresa web a revistei este http://
Comitetului de Etică al Universită ii, etc. În mod
similar, con rma i dacă experimentele asupra animalelor
trimestrial, articolele sunt acceptate în limba engleză sau
corespund standardelor etice.
română, având cel pu in traducerea în limba engleză a
rezumatului și cuvintelor cheie. Lucrările pot trimise
Asumarea dreptului de copyright
pe adresa: dr. Bumbulu Călin, editor șef adjunct,
Lucrările acceptate pentru publicare au implicit
Conexiuni Medicale, P- a. Eroilor Revolu iei nr. 23,
drepturile de copyright cedate către editor. Autorii pot
cod 440055, Satu Mare, România. Tel./Fax: +40-261-
utiliza materiale din lucrările lor în alte articole proprii,
710456, e-mail: bumbulutcalin@yahoo.com.
după ob inerea acceeptului editorului.
Republicarea articolelor
Propunerea pentru publicare
Vă rugăm să con rma i că lucrarea dumneavoastră
Toate manuscrisele propuse pentru publicare în
nu a mai fost publicată în forma prezentată sau într-o
Conexiuni Medicale vor în format compatibil pentru
formă asemănătoare, sau că nu a fost acceptată pentru
efectuarea recenziei online. Revista acceptă manuscrise
publicare într-o altă revistă.
propuse în formă electronică, în format Word (text,
guri și tabele). Nu trimite i lucrări în format PDF.
Conflicte de interese
Acceptăm lucrări care nu depășesc 3.500 de cuvinte
Rugăm autorii să declare posibilele con icte de
pentru articole originale, 2.500 pentru prezentări de
interese, inclusiv cele de natură nanciară. Dacă nu
caz, 2.000 pentru prezentări de imagini clinice, 500
există con icte de interese, vă rugăm să preciza i acest
pentru scrisori către editor și 4.500 de cuvinte pentru
lucru. Sursele de nan are trebuie precizate în lucrarea
reviste generale. Autorii NU vor trimite prin poștă sub
dumneavoastră.
formă de hârtie propunerea pentru publicare, decât
dacă este vorba de scrisori sau dacă se solicită astfel din
Permiterea de a reproduce materiale
partea redac iei. Dacă nu există altă op iune decât
publicate anterior
trimiterea prin poștă, vă rugăm să expedia i și versiunea
Vă rugăm să ne trimite i o copie a acceptului de
electronică CD-ROM pe adresa redac iei: Conexiuni
reproducere (de exemplu al ilustra iilor) de la de inătorul
Medicale, P- a. Eroilor Revolu iei nr. 23, cod 440055,
dreptului de copyright.
Satu Mare, România. Utiliza i text la două rânduri și
include i următoarele sec iuni: pagina de titlu,
Formularele de accept ale pacienților
rezumatul și cuvintele cheie, textul, mul umiri,
Protec ia drepturilor pacien ilor este esen ială; vă
referin e, tabele și guri. Paginile vor
numerotate
rugăm să ne trimite i formularele de accept ale
consecutiv, începând cu pagina de titlu, numerele
pacien ilor sau subiec ilor studiului dumneavoastră,
arabe ind plasate în col ul din dreapta sus al ecărei
prin care aceștia permit publicarea fotogra ilor sau altor
pagini.
123
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
Prezentarea lucrării
Nu recomandăm utilizarea excesivă a abrevierilor. Folosi i
Pagina de titlu
metode de calcul statistic standardizate. Nominaliza i
Cuprinde titlul întreg și titlul scurt format din
medicamentele și substan ele chimice utilizând numele
maxim 45 de caractere, numele și prenumele ecărui
generic
(dacă sunt men ionate mărcile înregistrate, se
autor; dacă lucrarea apar ine unui departament sau unei
furnizează numele producătorului și orașul).
institu ii, va men ionat numele acestuia în întregime.
Mul umiri
De asemenea numele, e-mail-ul și adresa autorului
Vor
adresate celor care au adus contribu ii
împuternicit pentru coresponden ă, sursele de nan are
importante la studiu.
sau suport utilizate sub forma burselor, echipamentelor,
Referin e
medicamentelor, sau orice combina ie a acestora.
Vor
numerotate între paranteze drepte cu
Rezumatul
numerale arabe, succesiv în ordinea în care sunt
Pagina a doua va cuprinde rezumatul cu minim 200
men ionate în text. Referin ele vor include numele
de cuvinte; nu utiliza i abrevieri, note de subsol, sau
autorilor până la al șaselea autor, dacă sunt mai mul i,
referin e.
enumera i primii trei și apoi adăuga i „et al”. Referin ele
Introducere în temă și scopuri
vor include titlul complet și sursa informa iei; numele
Descrie i importan a studiului și obiectivul
revistelor va abreviat conform Index Medicus (http://
(obiectivele) precise ale cercetării sau întrebarea
(întrebările) pe care le ridică studiul.
acceptă mai mult de 90-100 referin e; pentru scrisori
Metode
către redac ie se acceptă
5-6 referin e. Folosi i ca și
Include i informa ii privind următoarele aspecte ale
referin e cât mai pu ine rezumate. Comunicările
studiului dacă sunt utilizate: proiectul
- descrie i
personale și lucrările nepublicate nu vor men ionate la
elementele de bază ale studiului, de exemplu studiu
referin e și vor apare în text între paranteze. Lucrările
controlat randomizat, studiu cross-sec ional, de cohortă,
nepublicate dar a ate în curs de publicare vor incluse
de urmărire, serii de cazuri, etc; procedura - speci ca i
în referin e cu men iunea „in press” între paranteze,
dacă a fost desfășurat în sistem de îngrijire primar sau
lângă numele revistei implicate.
ter iar, în ambulator sau spital, în comunitate, etc;
a) Articole:
participan i - indica i numărul subiec ilor și cum au
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
fost selecta i, recruta i și desemna i pentru interven ie;
MA, Holub MC, Kovalsykz I, et al. Toward understanding
interven ia
- metoda de administrare și durata
the role of leptin and leptin receptor antagonism in
interven iei.
preclinical models of rheumatoid arthritis. Peptides
Rezultate
2011;32:1567-74.
Prezenta i principalele rezultate ale studiului,
b) Lucrări publicate numai cu numerele DOI:
inclusiv intervalurile de con den ă sau valorile p.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
Concluzii
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Enun a i doar concluziile sus inute direct de dovezi,
vascular periadventitial adipose tissue (tunica adiposa) as
precum și importan a descoperirilor. Revistele generale
an example. Cell Biol Int
2011;doi:
10.1042/
și prezentările de caz vor include un rezumat
CBI20110422.
nestructurat.
c) Căr i sau manuale:
Cuvinte cheie
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Rezumatul va urmat de o listă de 3-10 cuvinte
Landes Bioscience, Austin, Texas, USA. 2009.
cheie sau fraze scurte care vor ajuta la indexare. Dacă
d) Capitole de căr i sau de manuale:
este posibil, utiliza i termeni proveni i din lista Index
[4] Jeremy L, Abe PD. Treatment Options in
Medicus cu
262 subiecte medicale/Medical Subject
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
Headings
262
cancers in clinical practice, Springer-Verlag, London
meshhome.html).
Limited, 2007:75-102.
Textul
Tabele
Un studiu original va divizat în sec iuni denumite
Fiecare tabel va numerotat cu numerale romane,
Introducere, Metode, Rezultate și Discu ii
(incluzând
cu un titlu scurt deasupra, la subsolul lor vor trecute
concluziile), după formula „IMRAD”. Articolele lungi
notele
explicative,
men ionându-se abrevierele
pot necesita subsec iuni (în special la Rezultate și Discu ii)
nestandardizate utilizate; nominaliza i valorile statistice
pentru clari care. Alte tipuri de articole precum prezentări
care variază precum devia ia standard și eroarea standard
de caz, reviste generale, editoriale, pot urma alt format.
a medianei. Fiecare tabel va citat în text.
124
MEDICAL CONNECTIONS • NUMBER 1 (33) • MARCH 2014
GUIDANCE FOR DRAWING UP
Figuri
acestor sugestii, rugându-i să răspundă la întrebări și să
Toate gra cele, fotogra ile, diagramele vor
facă necesarele corec ii. Aceste informări sunt făcute în
considerate ca guri și vor numerotate succesiv în text
cel mult trei luni de la propunerea de publicare.
cu numerale arabe. Dacă o gură a fost publicată
Manuscrisul revizuit de autori va reexpediat editorului
anterior, sursa va citată cu mul umiri, men ionându-
în cel mult o lună. La primirea de către editor a versiunii
se permisiunea de inătorului de copyright. Figurile pot
corectate, înso ită de o scrisoare de răspuns punctuală la
reduse, grupate sau șterse la dorin a editorului.
comentariile recenzorilor, se retrimite manuscrisul
Legenda gurii va plasată la subsolul ei; va explicată
acelorași recenzori, care vor face recomandarea nală
scala utilizată, respectiv metodele de colorare
pentru acceptarea sau respingerea acestuia.
microscopică.
Unită i de măsură
Abonamente
Măsurătorile lungimii, înăl imii, greută ii și
Pre ul unui abonament anual pentru 2014 este: 80
volumului vor făcute în sistem metric sau multipli
RON individual, 160 RON pentru institu ii, plăti i în
decimali. Temperaturile vor
exprimate în grade
contul Colegiului Medicilor Satu Mare RO38 BTRL
Celsius. Tensiunea va
măsurată în mmHg. Toate
0310
1202 K392
62XX, cod scal
9839430, cu
măsurătorile hematologice vor exprimate în Sistemul
men iunea
„pentru abonament Conexiuni Medicale”.
Interna ional de Unită i (SI).
Solicitarea abonării poate
trimisă prin poștă: P- a.
Abrevieri și simboluri
Eroilor Revolu iei nr.
23, cod
440055, Satu Mare,
Utiliza i doar abrevieri standard. Evita i abrevierile
România. Tel./Fax: 0261-710456, 0361-408164, sau
în titlu și rezumat. Cuvântul va preceda abrevierea la
prin e-mail: colmedsm@gmail.com.
prima utilizare în text, cu excep ia unită ilor de măsură
standard.
Publicitate
Cererile pentru spa iu publicitar vor
adresate
Retipăriri
redac iei Conexiuni Medicale. Pre urile (plătite în lei la
Sunt oferite gratuit zece copii ale articolului publicat
cursul BNR) pentru publicitate pe 2014 sunt 200 euro
și două ale revistei. Dacă sunt necesare mai multe copii,
pagina (A4) color, un număr și 800 euro patru numere;
sunt disponibile contra cost.
coperta interioară fa ă sau spate: 350 euro un număr,
1400 euro patru numere; coperta exterioară spate: 400
Politica editorială
euro un număr, 1600 euro patru numere. Cont bancar:
Apreciem toate contribu iile în domeniul medicinei.
Colegiul Medicilor Satu Mare, CUI 9839430, Banca
Invităm personalită i recunoscute cu expertiză și articole
Transilvania, agen ia Golescu Satu Mare, IBAN: RO38
din diverse domenii să publice reviste generale și
BTRL 0310 1202 K392 62XX.
editoriale în revista noastră. Acceptăm de asemenea
lucrări originale și prezentări de caz din toate ările.
© Copyright Conexiuni Medicale/Medical
Conexiuni Medicale vă oferă o recenzie atentă și publicarea
Connections, Satu Mare, 2014
imediată după acceptare. Redactorii vor citi primii
Nicio parte a acestei publica ii nu poate reprodusă,
lucrarea, decizând în decurs de 1-3 săptămâni în func ie
stocată sau transmisă sub orice formă sau prin orice
de nivelul de prioritate: unele sunt trimise imediat
mijloace, fără permisiunea prealabilă în scris a revistei
recenzorilor, unele pot
respinse, iar unele sunt
Conexiuni Medicale. Permisiunea nu este necesară
returnate autorilor cu sugestii de îmbunătă ire înainte
pentru a copia rezumate sau articole dacă este indicată
de expedierea spre recenzori.
sursa, cu citarea completă a referin ei. Solicitarea
privind permisiunea de a retipări toată revista sau o
Procedura peer-review
parte a ei, va
adresată editorului prin e-mail:
Conexiuni Medicale practică o evaluare a tuturor
colmedsm@gmail.com
lucrărilor originale de către doi sau trei recenzori
independen i, din care doi sunt personalită i
Revista Conexiuni Medicale apare trimestrial prin
interna ionale. Procesul peer-review este esen ial pentru
efortul logistic și nanciar al Colegiului Medicilor
asigurarea calită ii informa iei știin i ce. Recenzorii
Satu Mare și Asocia iei Medicilor de Familie Satu
sunt ruga i să evalueze manuscrisul aplicând aceleași
Mare, în cadrul proiectului comun al Centrului de
standarde ca și pentru reviste interna ionale; comentariile
Documentare și Educa ie Medicală Continuă Satu
sunt trimise editorului, care va informa autorii asupra
Mare.
125